While working on this page, I came across a saving opportunity in R – save.image. It was a fantastic possibility till it was not anymore. After opening R and pressing save.image left me with an empty workspace and hours of lost work. Hence this page is not complete yet.
These tables show the complex (theoretical) interplay between the hormones.
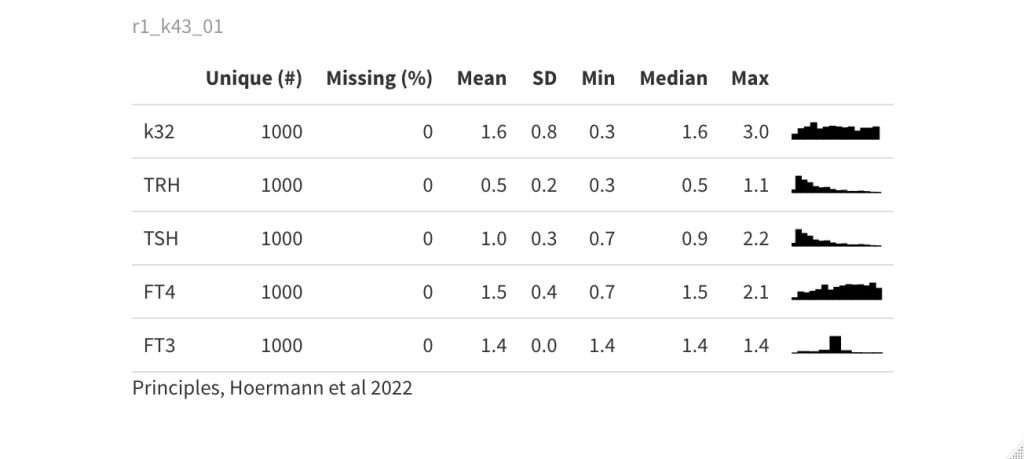
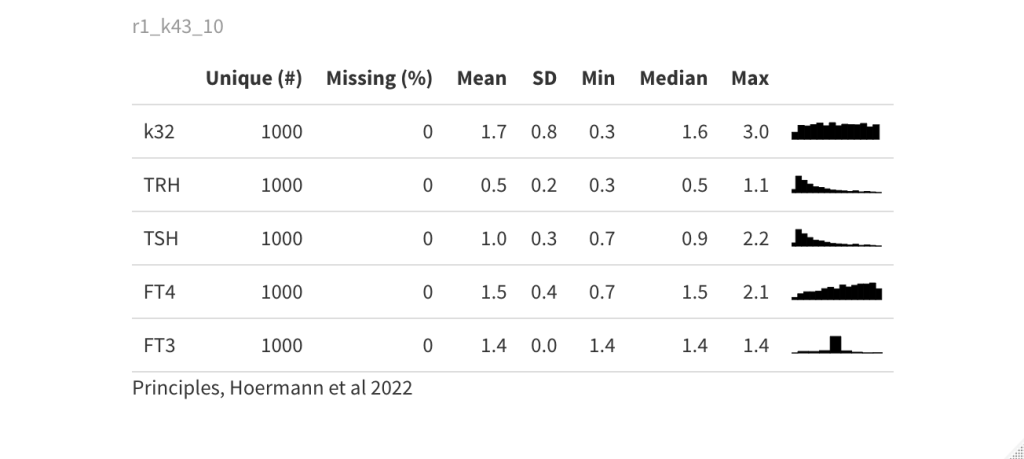
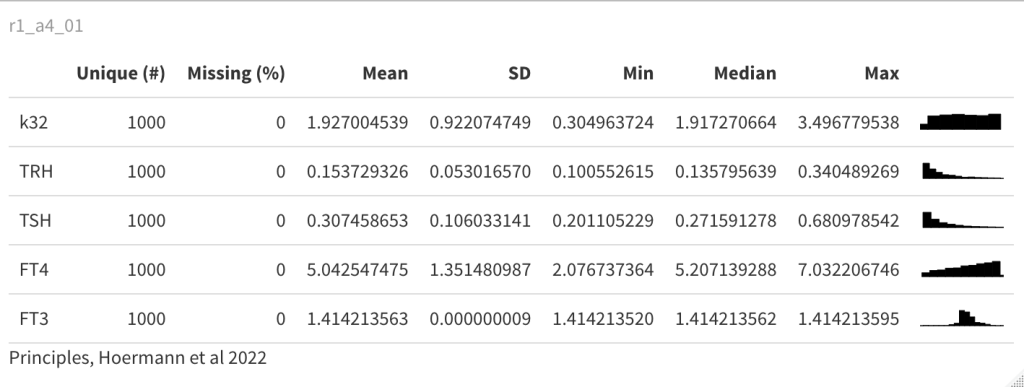
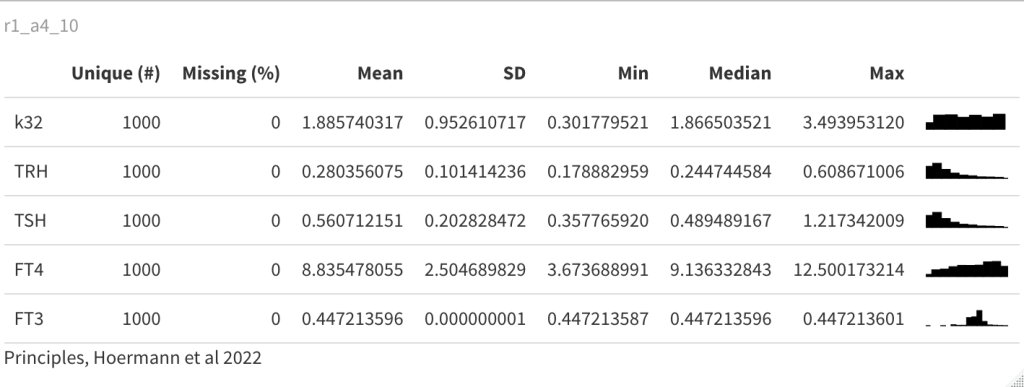
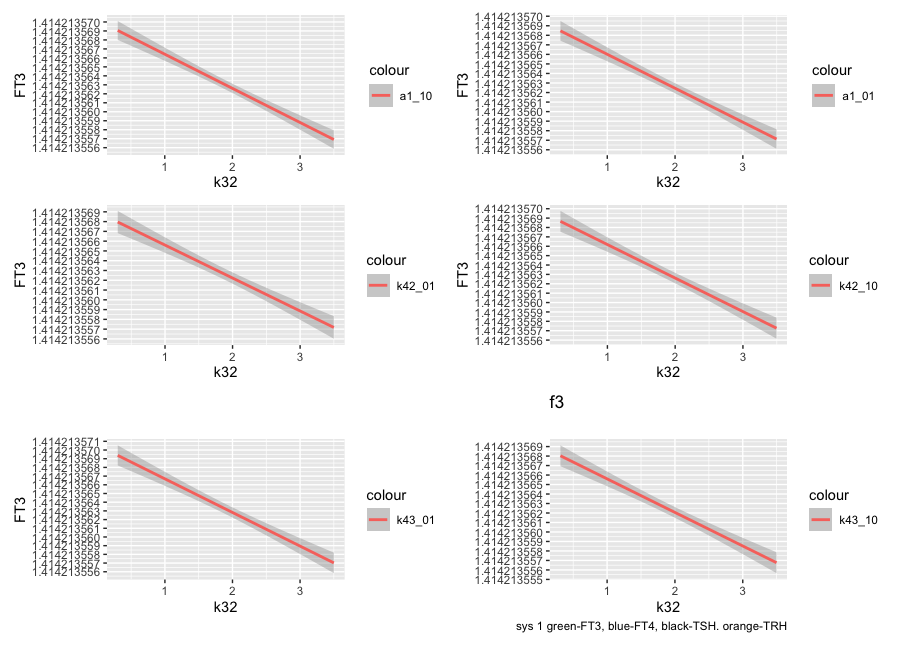
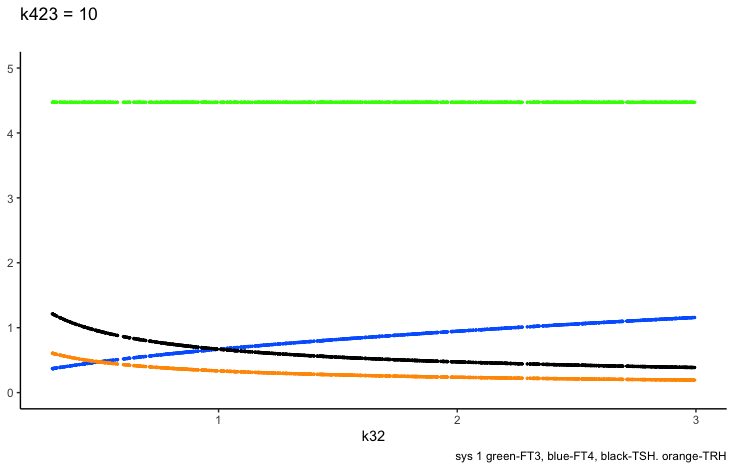
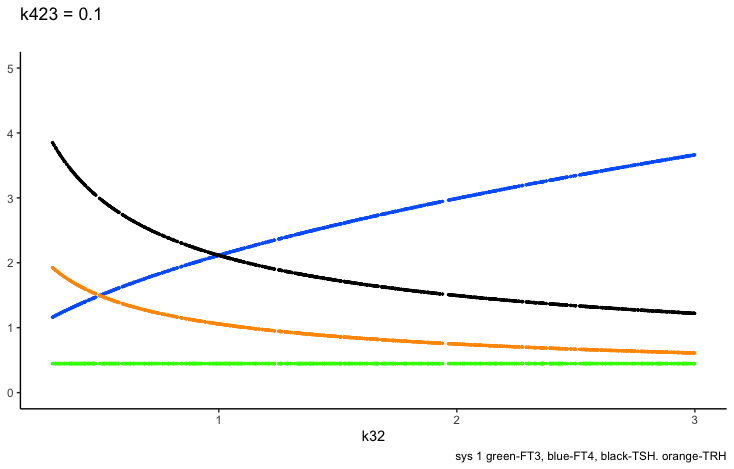
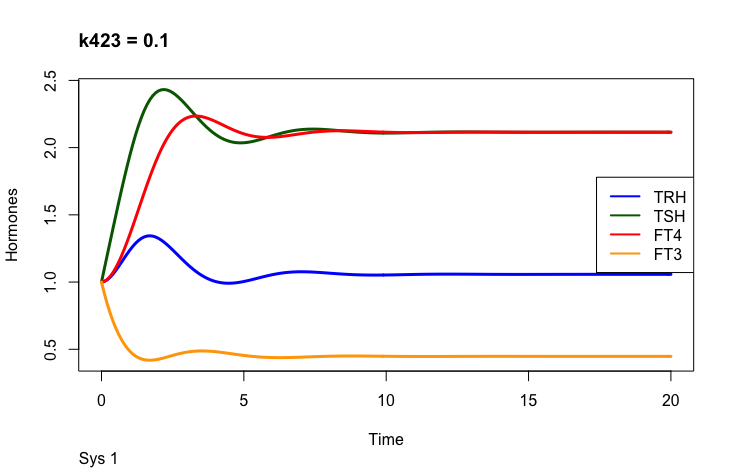
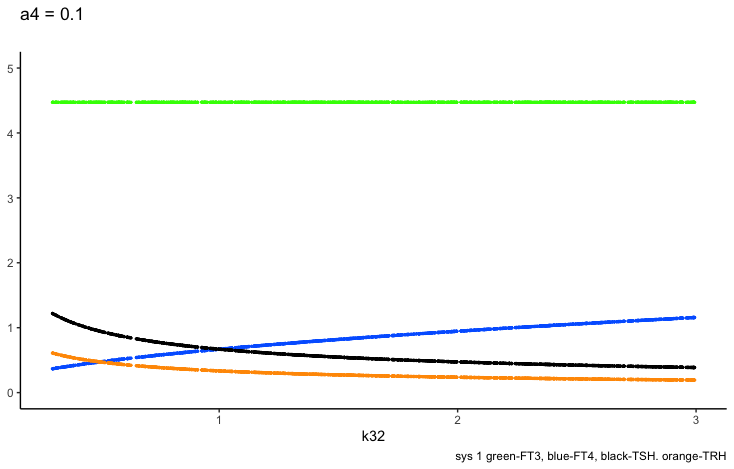
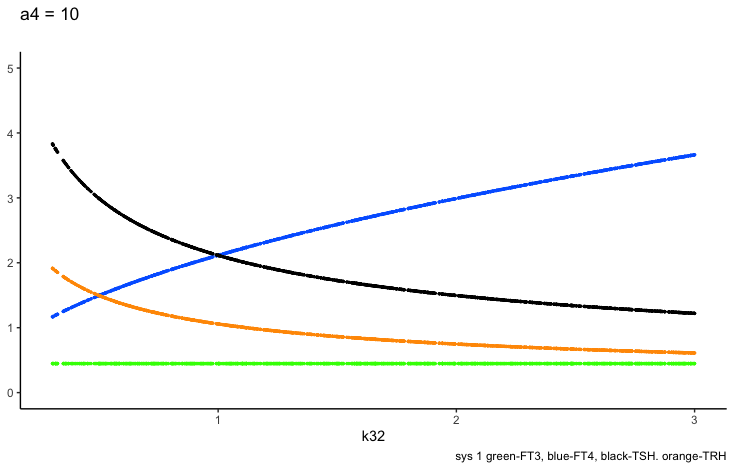
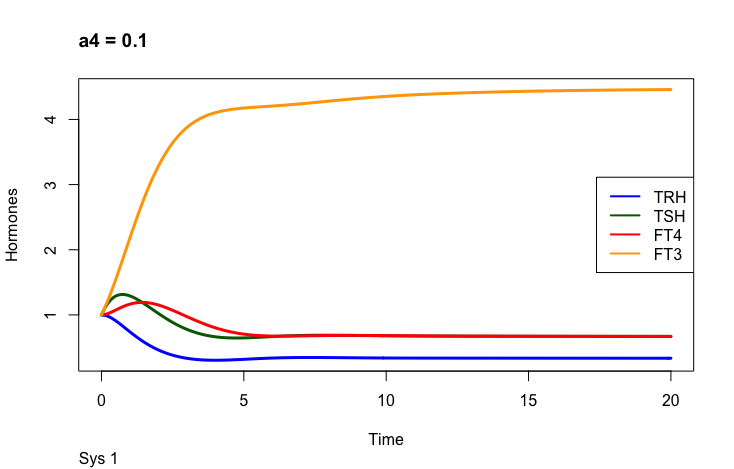
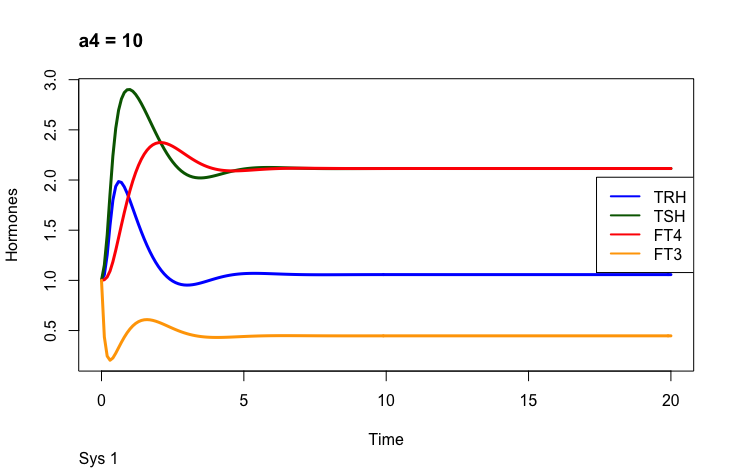
Two parameters may change the value of FT3 in the mathematical model (Ref.1); k423 – positive feedforward of TSH and FT4 onto FT3 (downstream, activating) a4 – the FT3 elimination rate constant.
Only examples of the effect of the parameter –
Hoermann R, Pekker MJ, Midgley JEM, Larisch R and Dietrich JW (2022) Principles of Endocrine Regulation: Reconciling Tensions Between Robustness in Performance and Adaptation to Change. Front. Endocrinol. 13:825107. doi: 10.3389/fendo.2022.825107 https://www.frontiersin.org/articles/10.3389/fendo.2022.825107/full
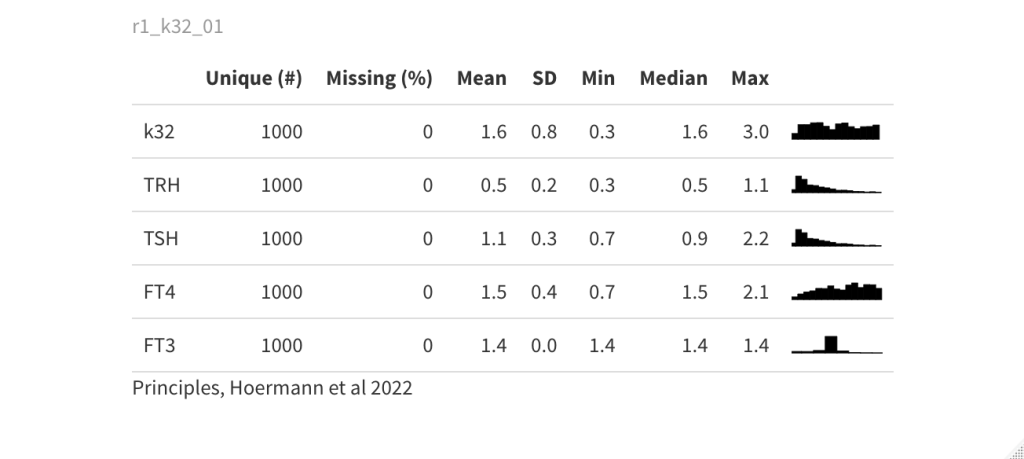
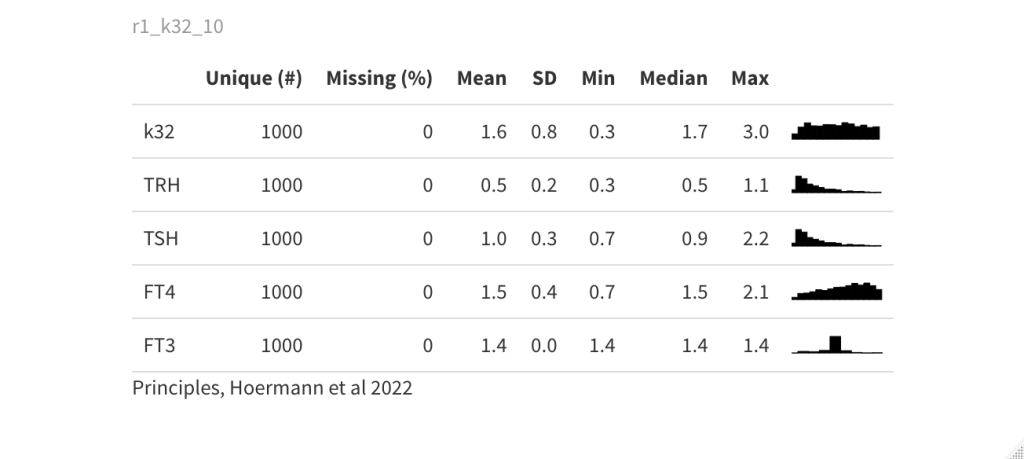
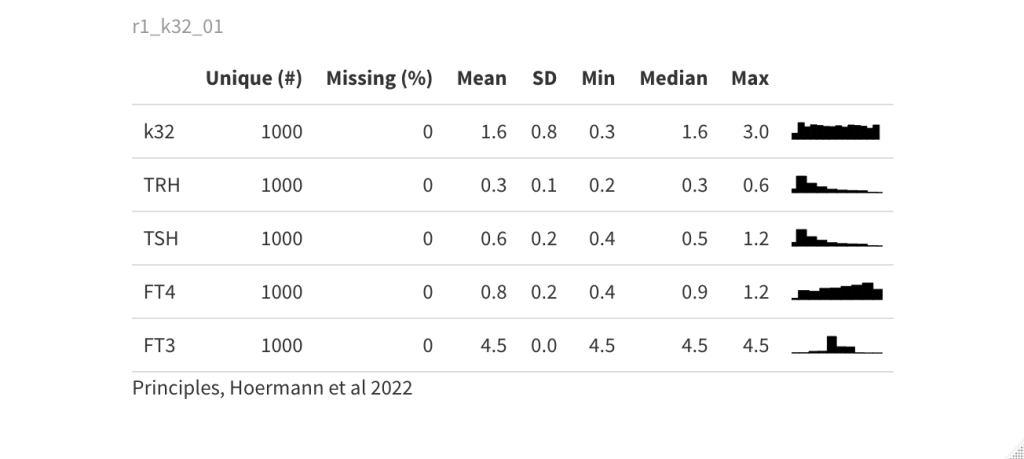
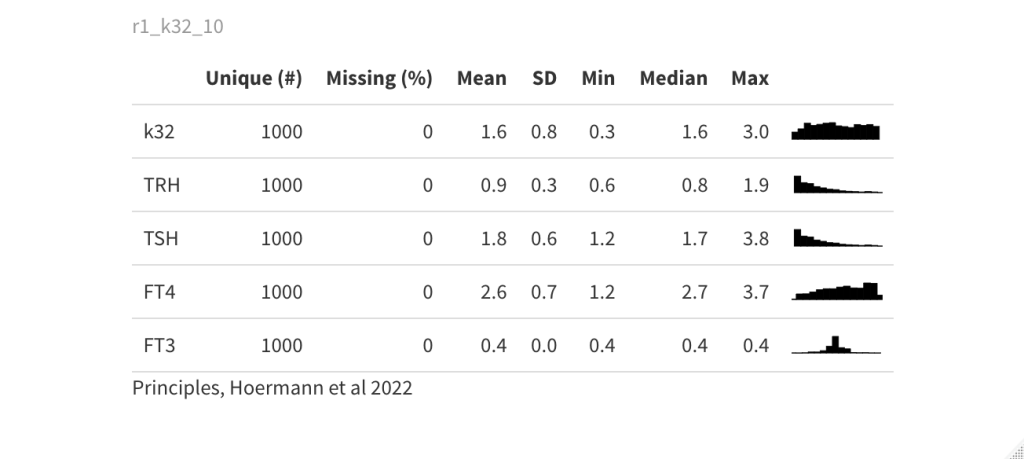
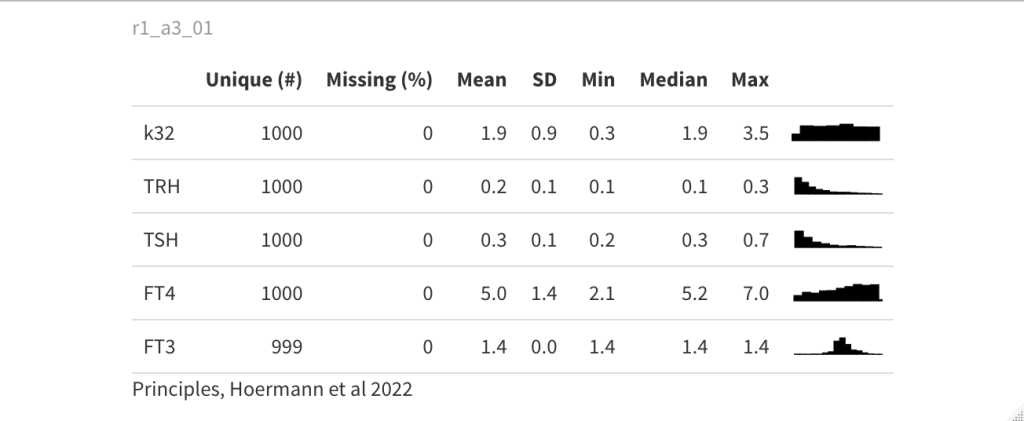
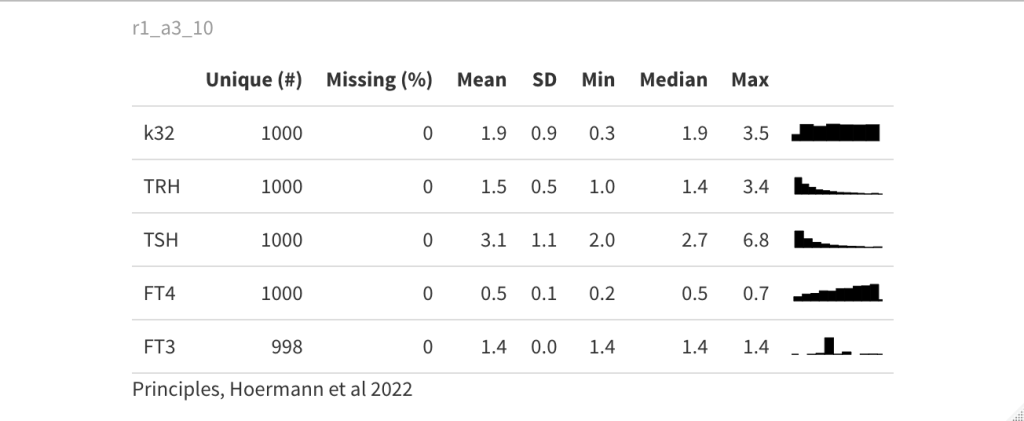
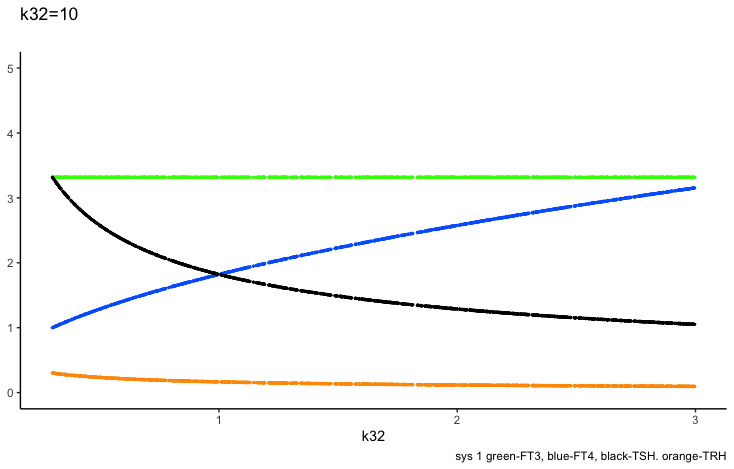
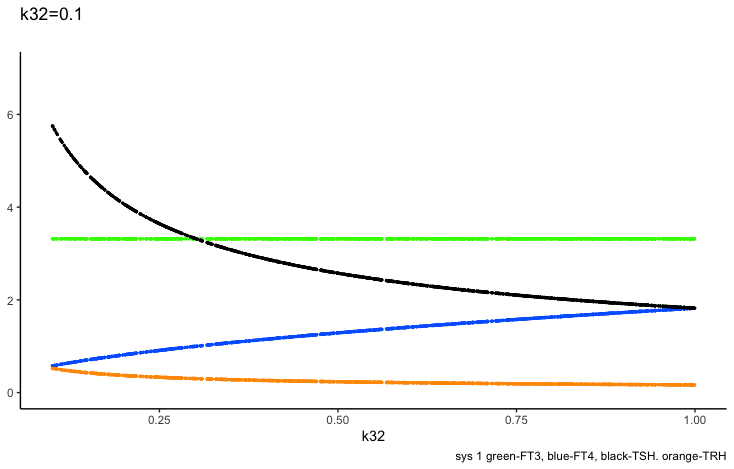
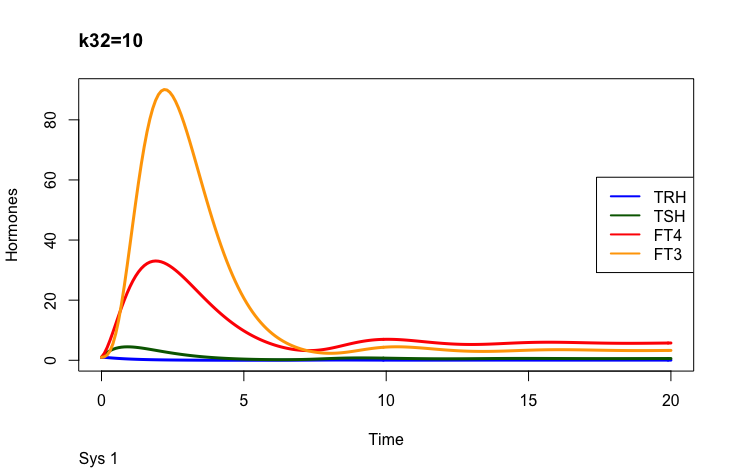
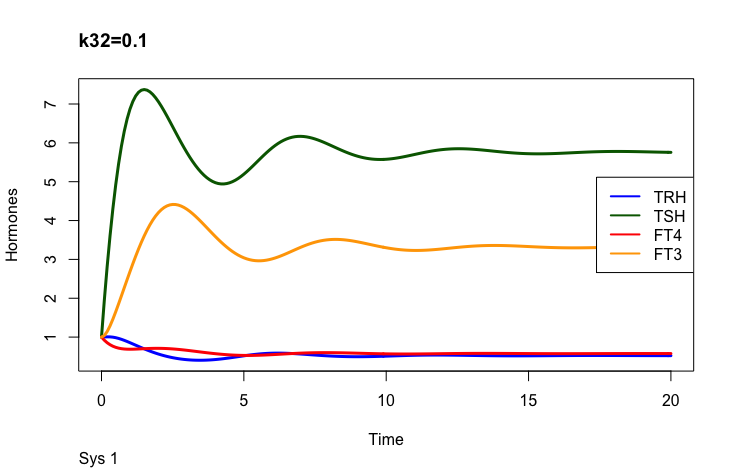
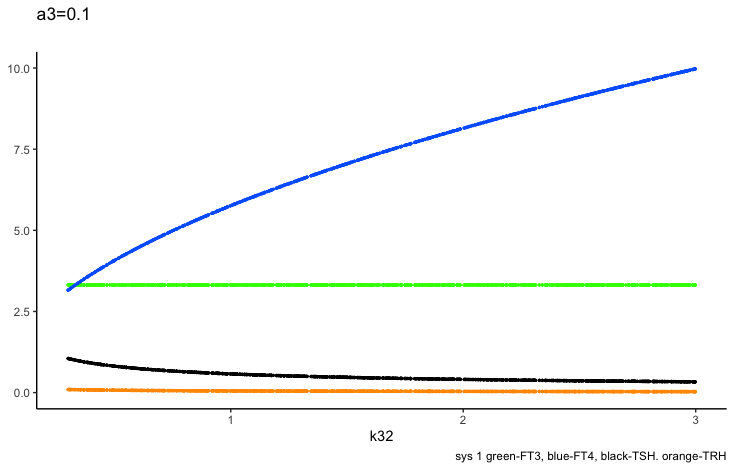
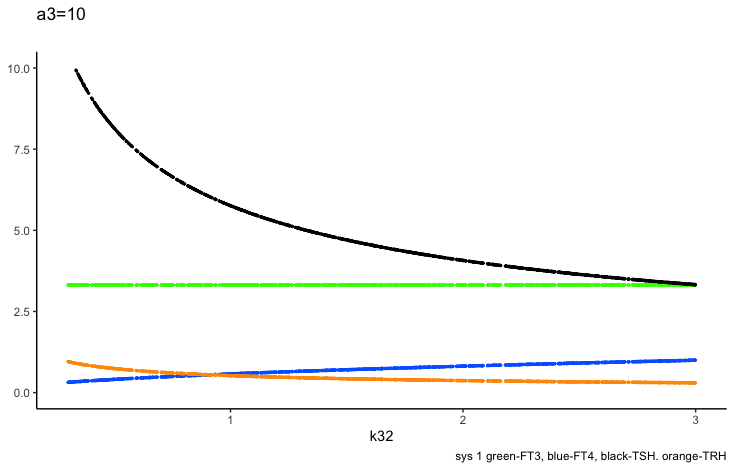
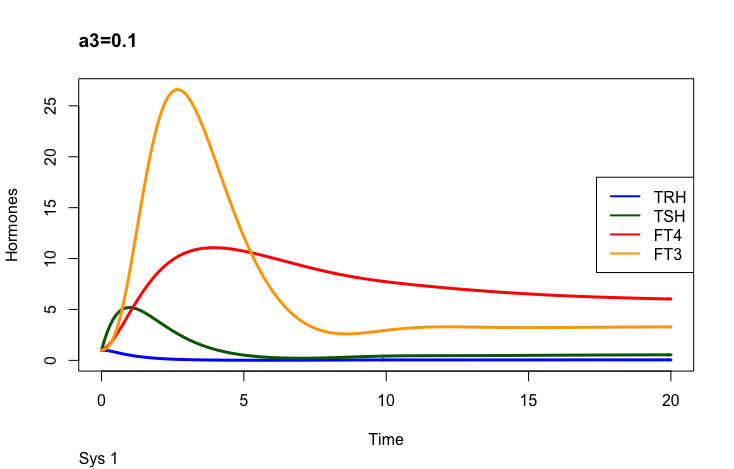
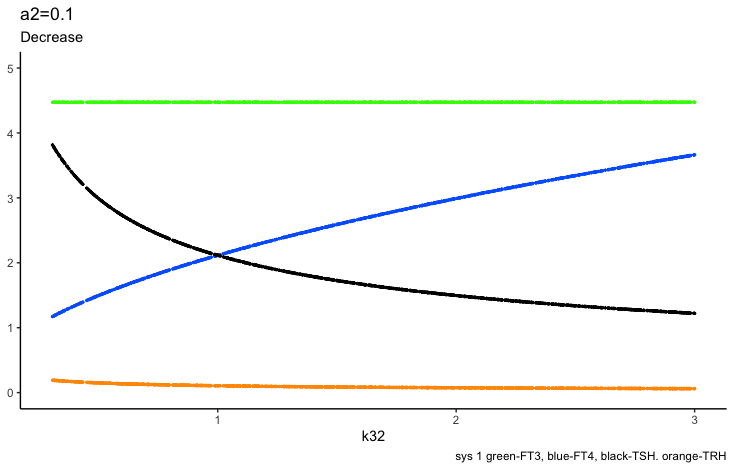
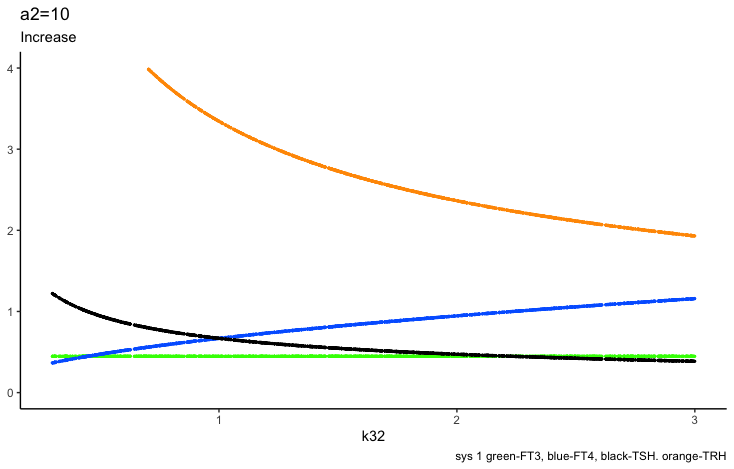
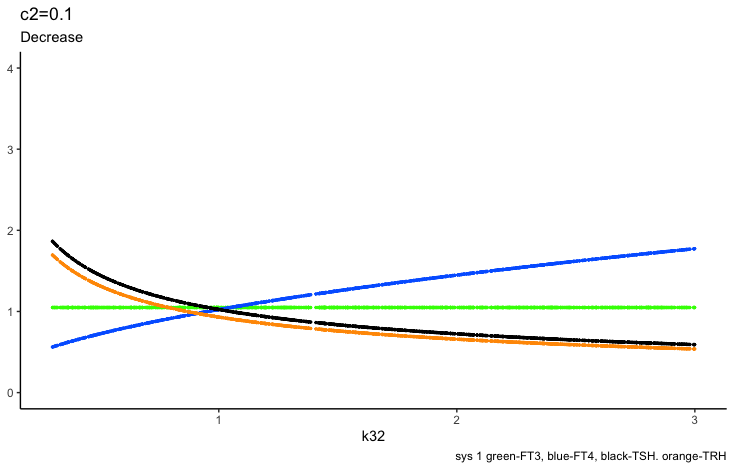
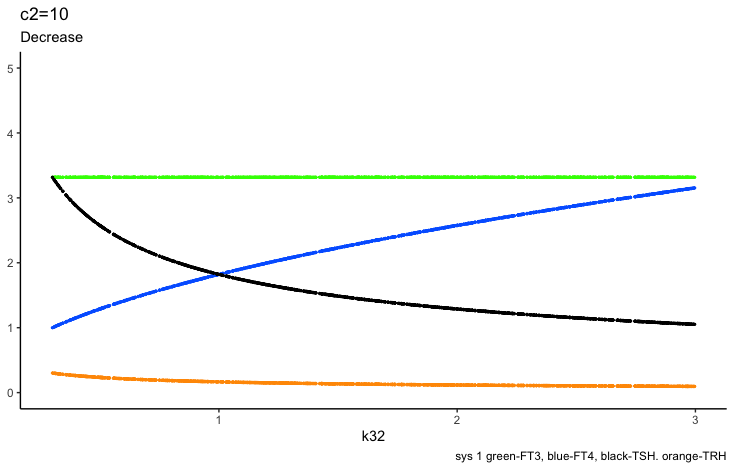
In the mathematical model (Ref. 1) two parameters may change the outcome of FT4: k32 – positive feedforward of TSH onto FT4 (downstream, activating) and a 3 – the FT4 elimination rate constant.
Sense?
Only examples of the effect of the parameter –
Hoermann R, Pekker MJ, Midgley JEM, Larisch R and Dietrich JW (2022) Principles of Endocrine Regulation: Reconciling Tensions Between Robustness in Performance and Adaptation to Change. Front. Endocrinol. 13:825107. doi: 10.3389/fendo.2022.825107 https://www.frontiersin.org/articles/10.3389/fendo.2022.825107/full
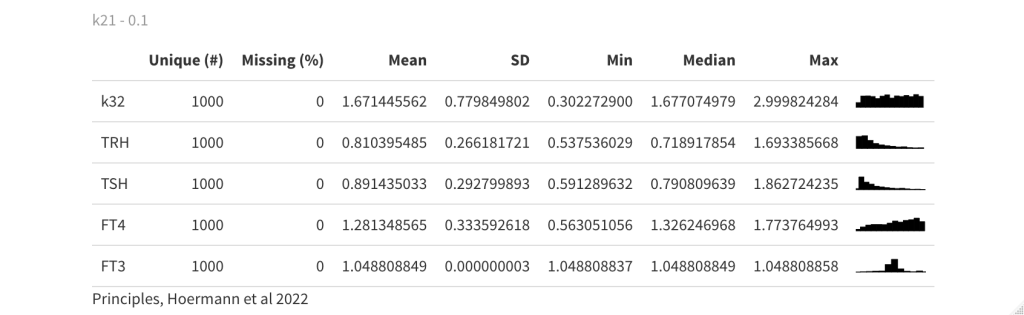
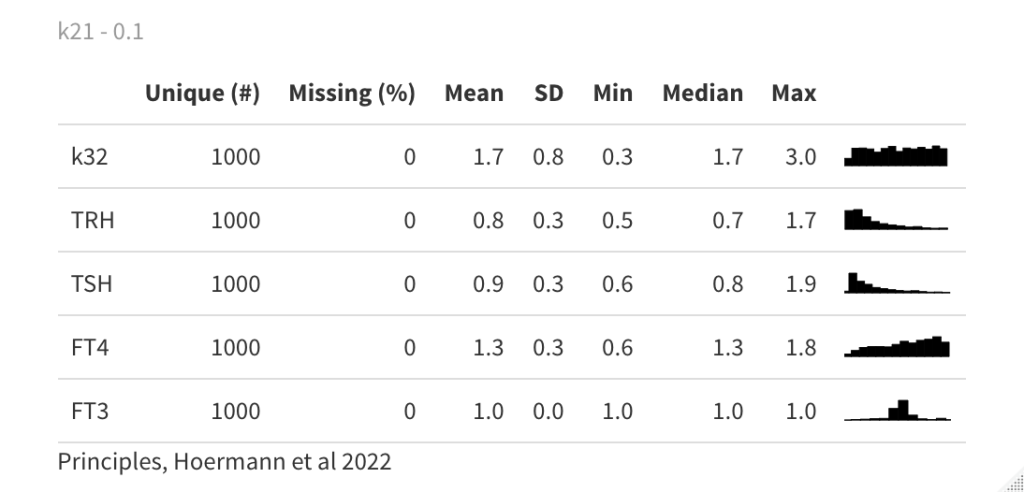
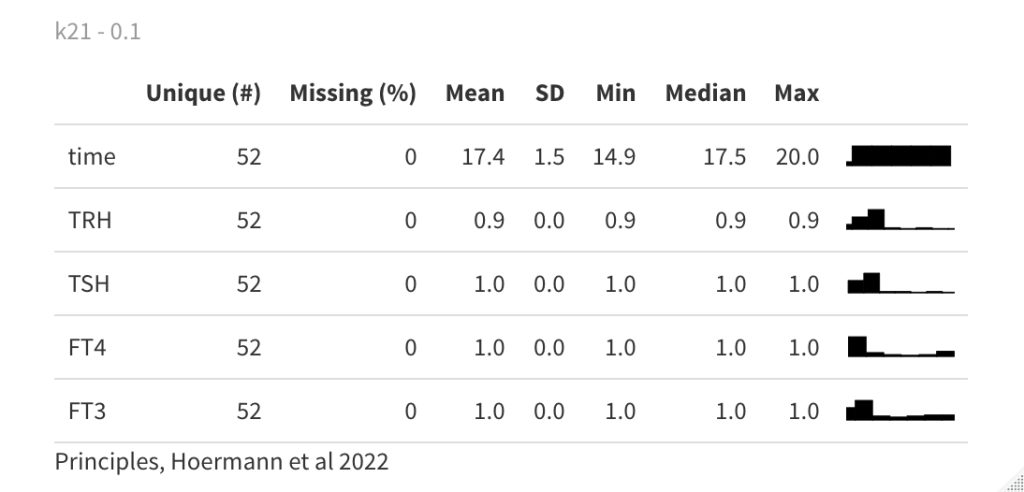
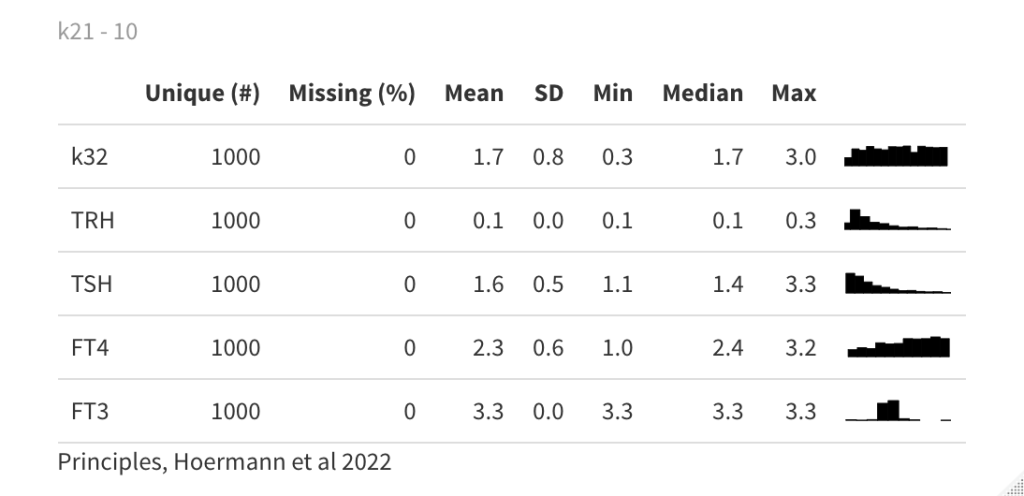
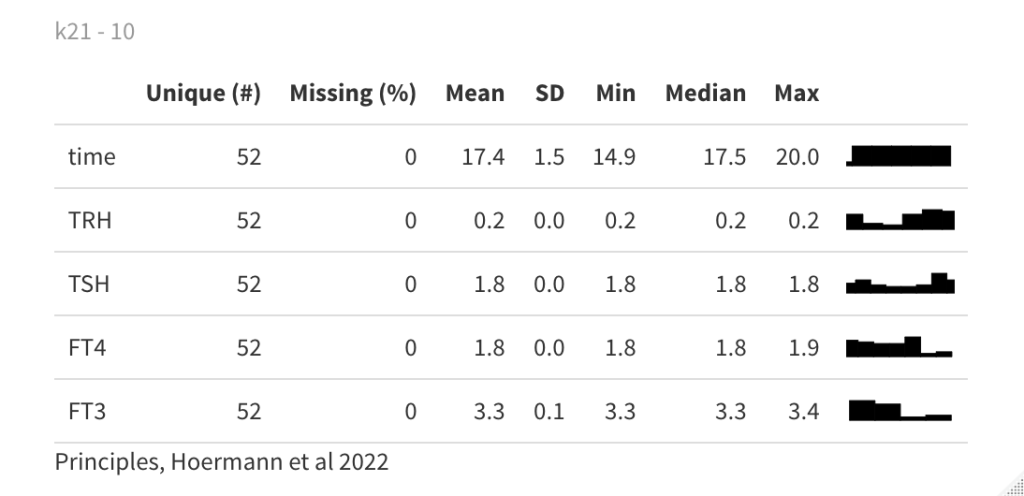
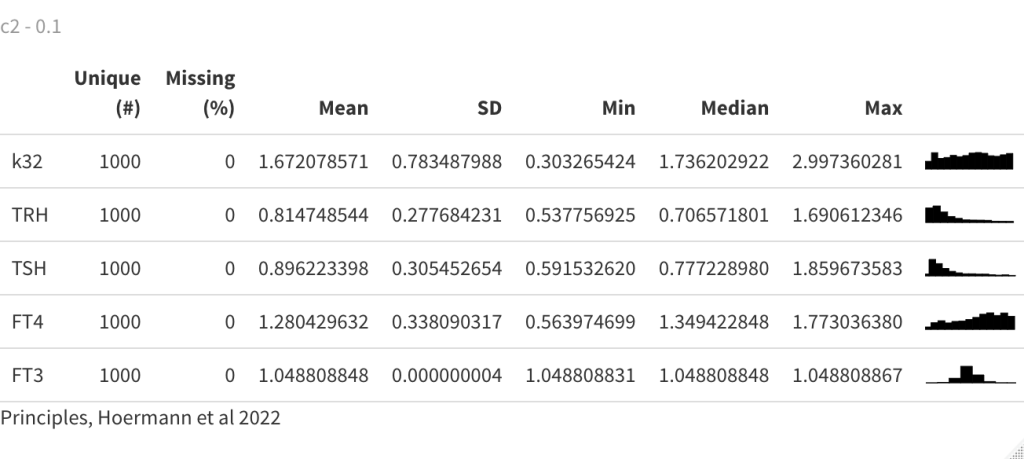
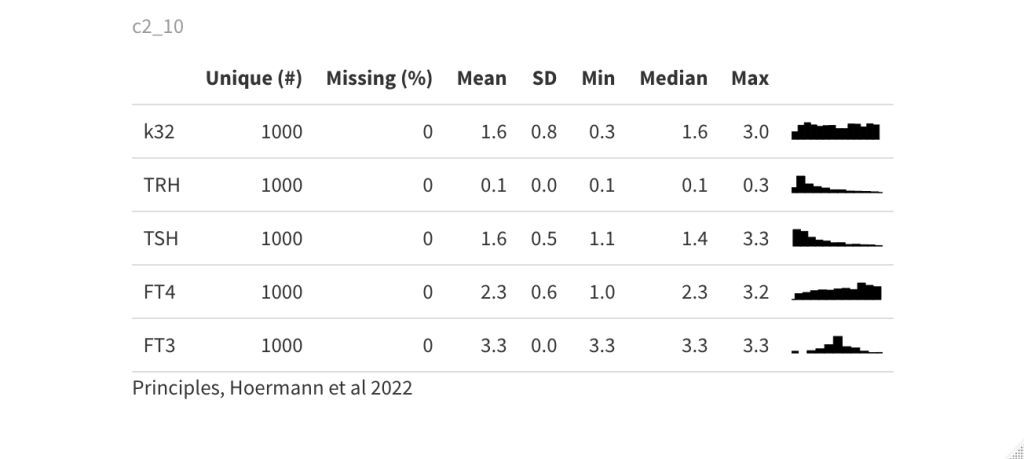
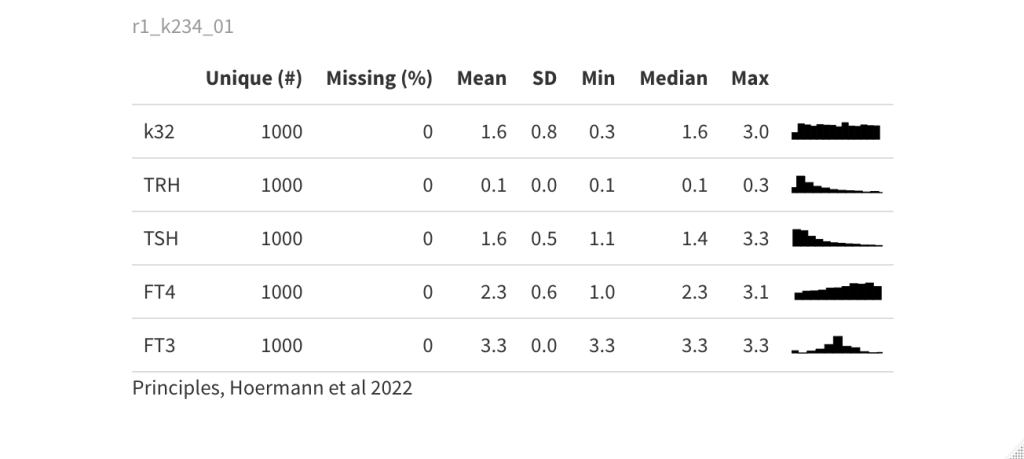
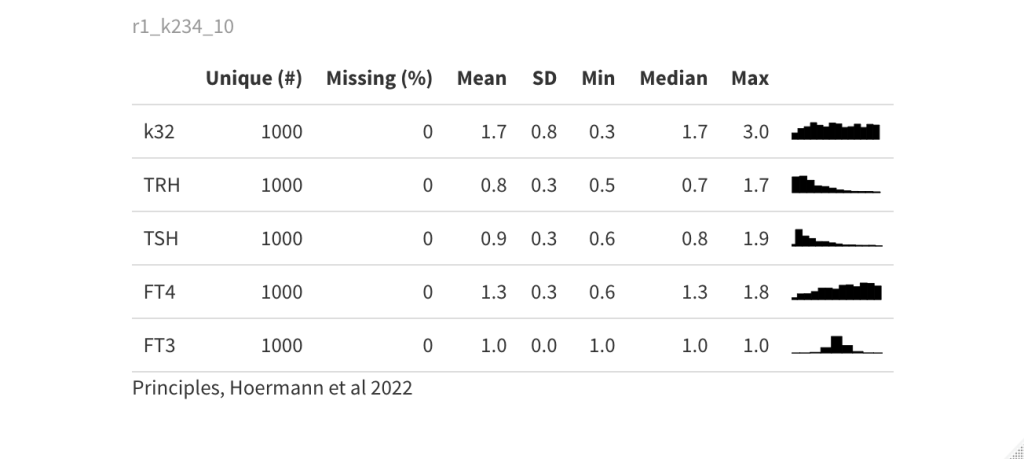
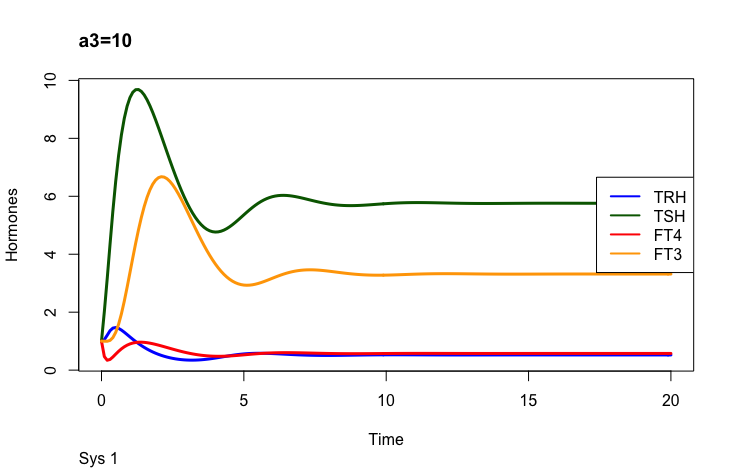
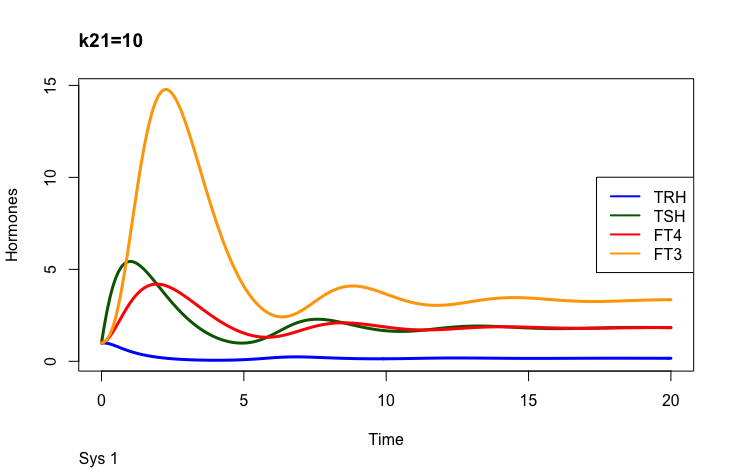
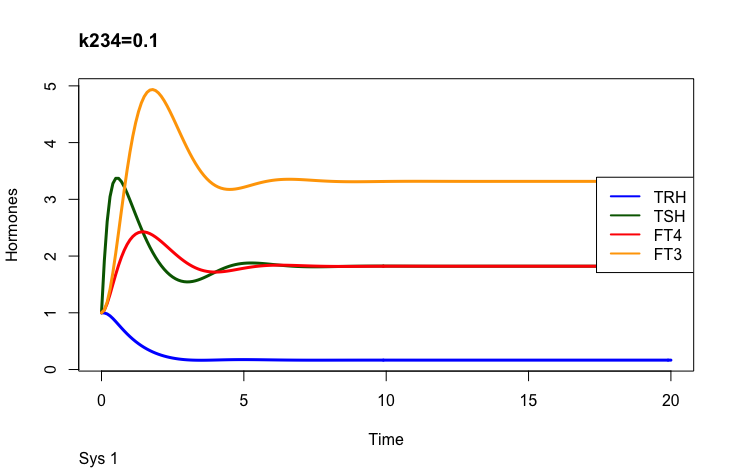
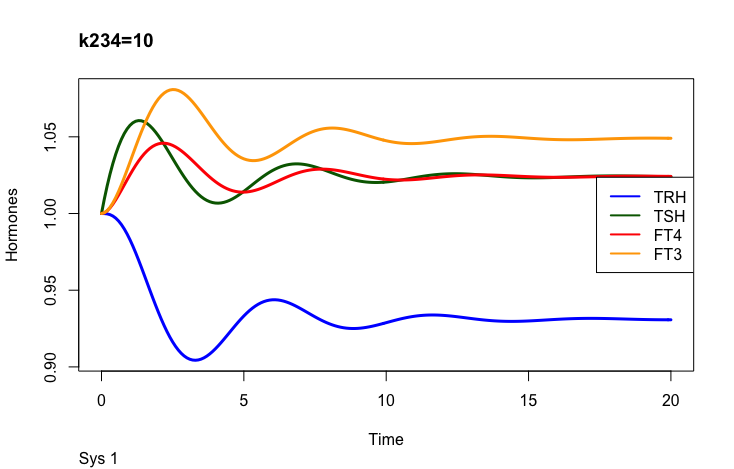
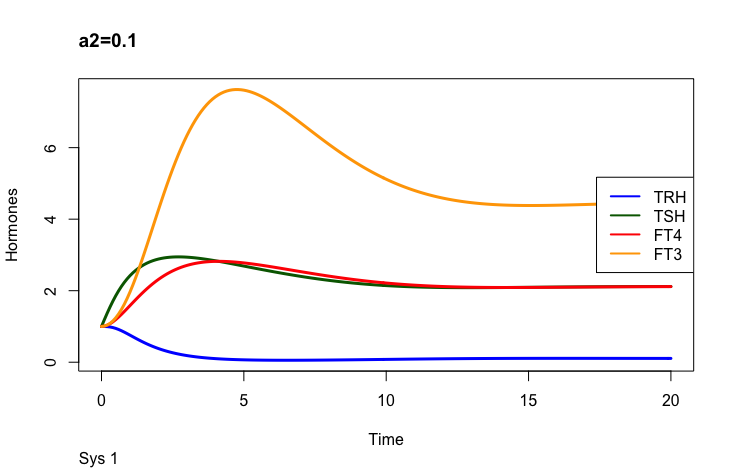
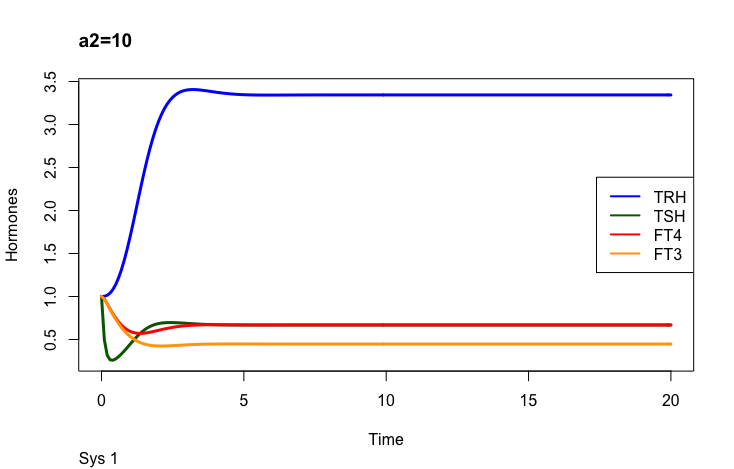
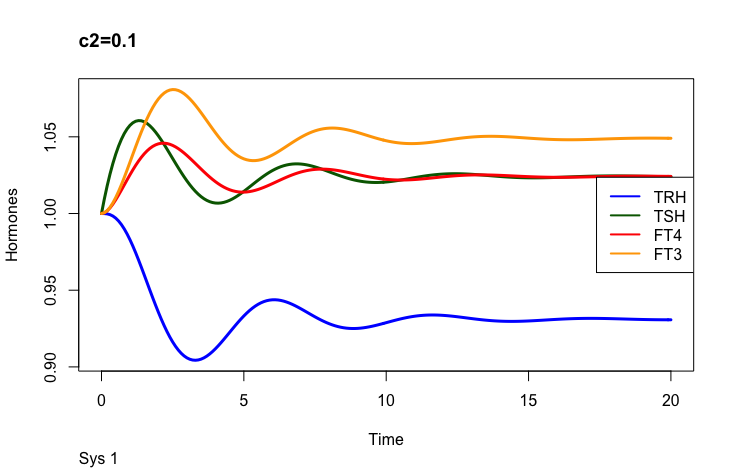
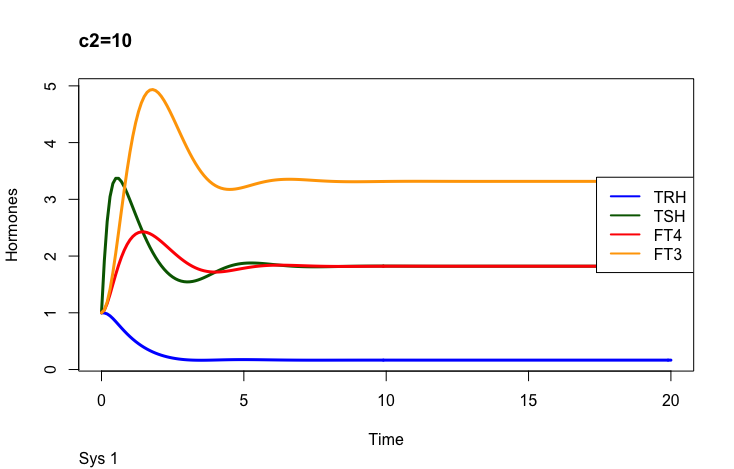
Four parameters regulate TSH (in the mathematical model (ref.1)): k21 – (positive feedforward of TRH onto TSH (downstream, activating)), c2 – (the secretory capacity constant), k234 -negative feedback of FT4 and FT3 onto TSH (upstream, repressing) and a2 – (the TSH elimination rate constant.).
Be aware that the colours for the hormones are different in the rows below.
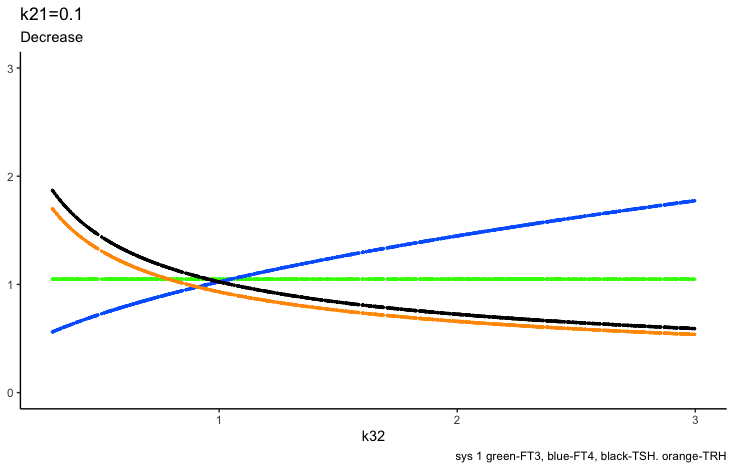
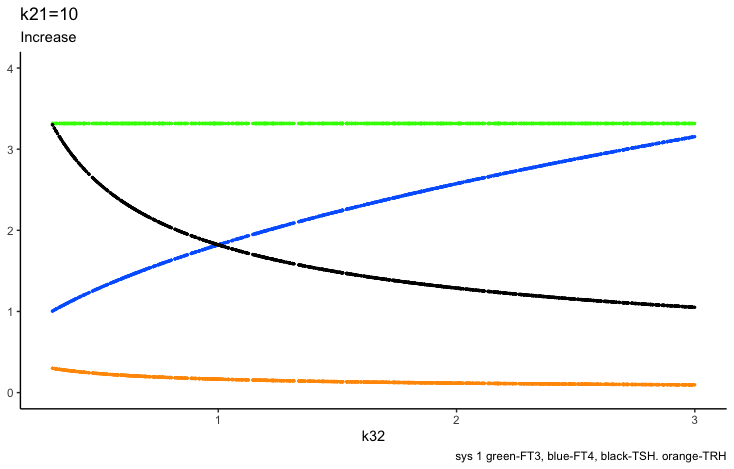
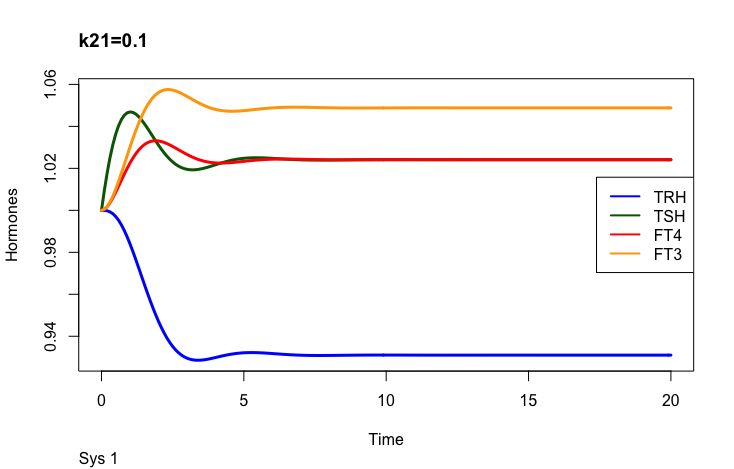
Positive feedforward of TRH onto TSH (downstream, activating)):
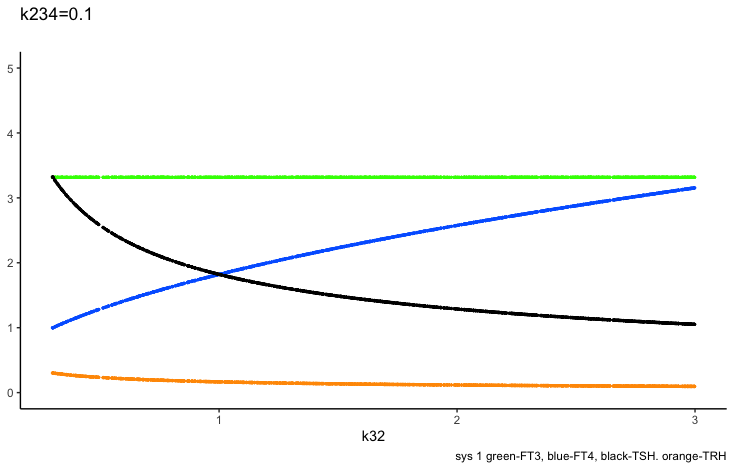
Level compared to the equilibrium calculation
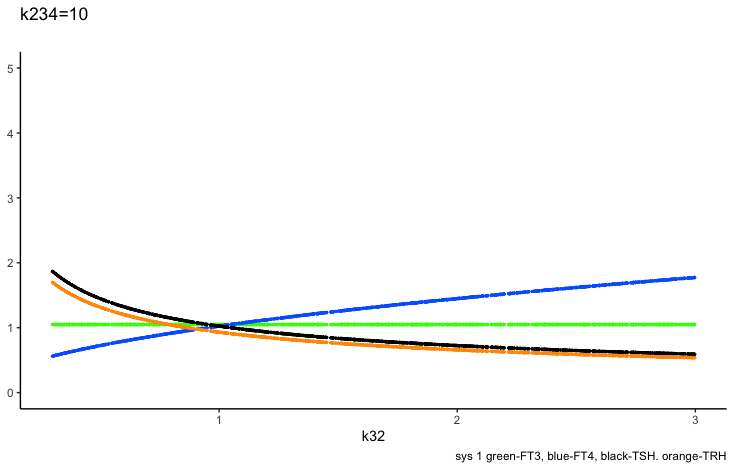
Negative feedback of FT4 and FT3 onto TSH (upstream, repressing)
The TSH elimination rate constant.
The secretory capacity constant
Only examples of the effect of the parameter –
Hoermann R, Pekker MJ, Midgley JEM, Larisch R and Dietrich JW (2022) Principles of Endocrine Regulation: Reconciling Tensions Between Robustness in Performance and Adaptation to Change. Front. Endocrinol. 13:825107. doi: 10.3389/fendo.2022.825107 https://www.frontiersin.org/articles/10.3389/fendo.2022.825107/full
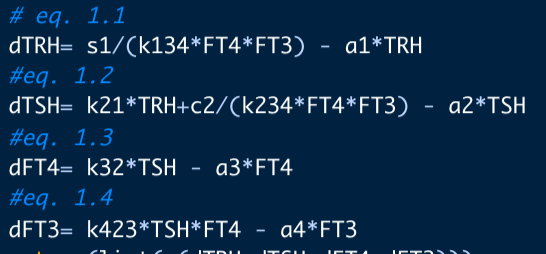
Hoerman et al (Ref.1) have developed a mathematical model with 14 different parameters that influence the HPT axis (hypothalamus – pituitary – thyroid axis). I will describe the effects in the following.
There are different parameters which can change the hormones in this mathematical model.
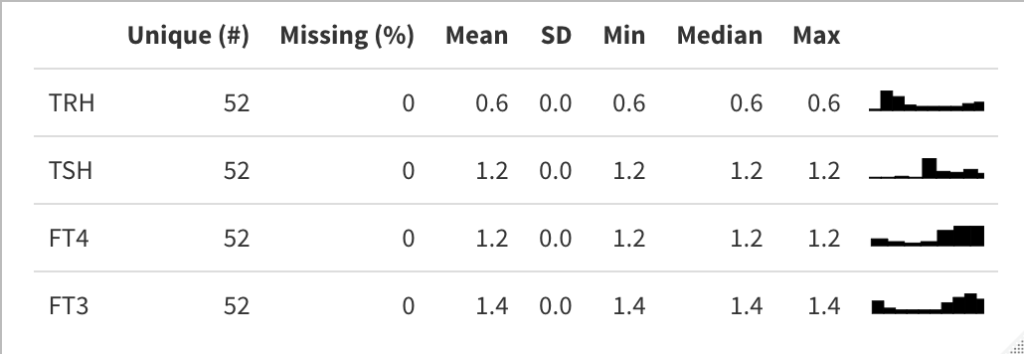
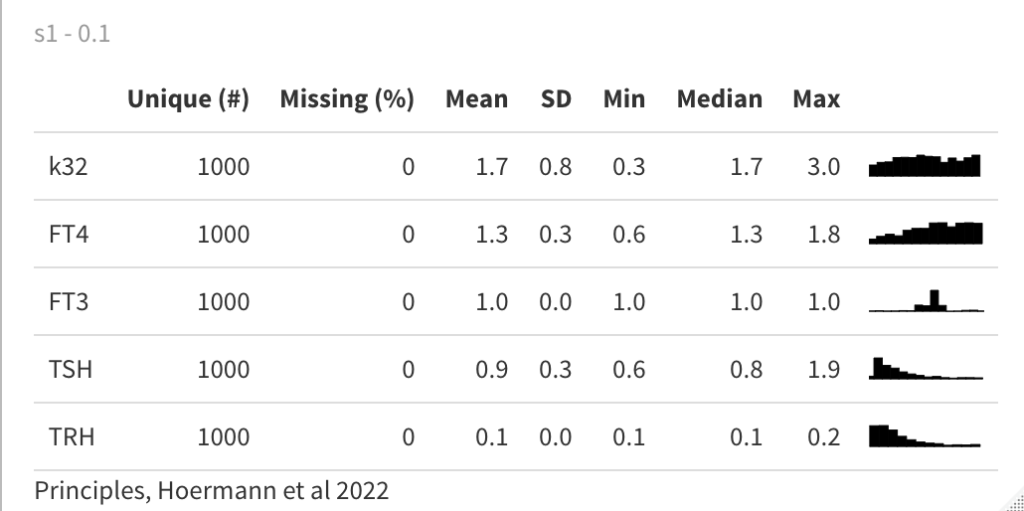
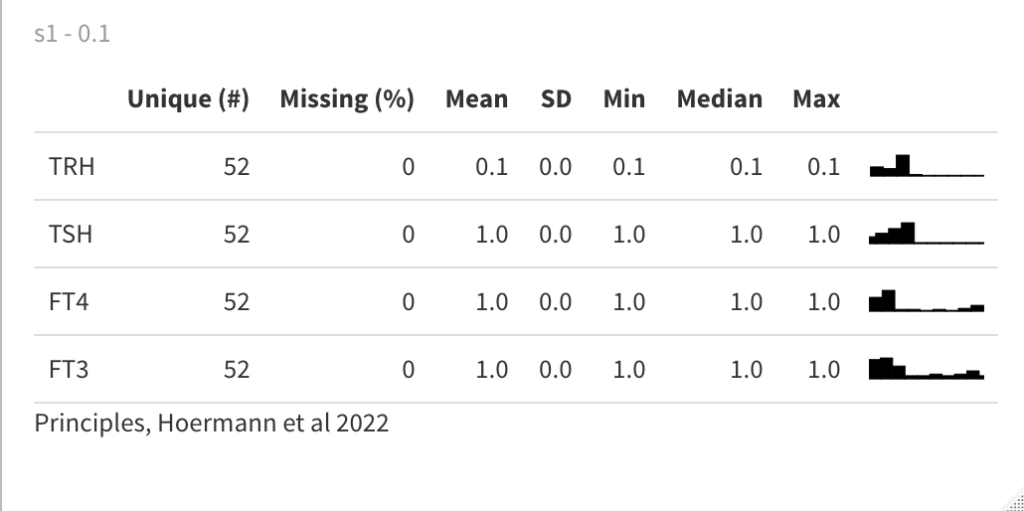
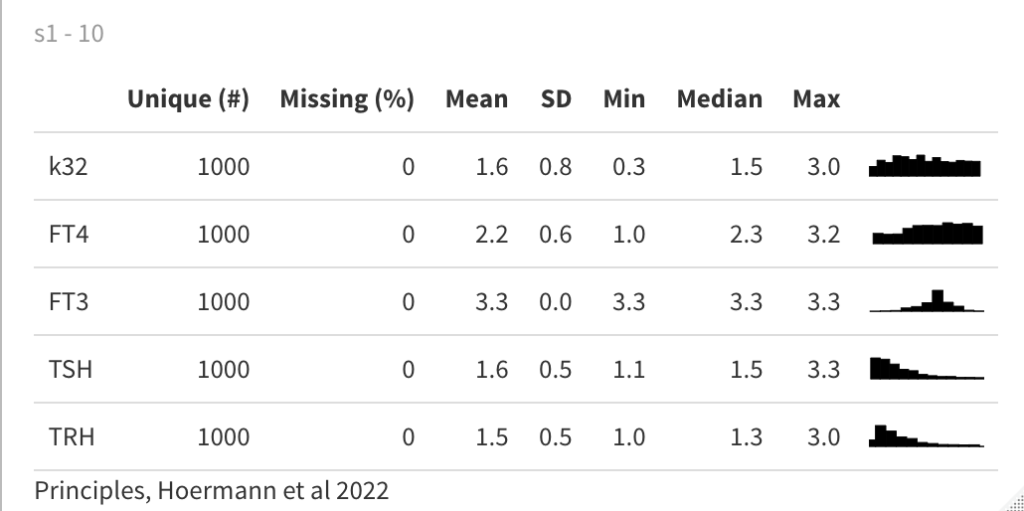
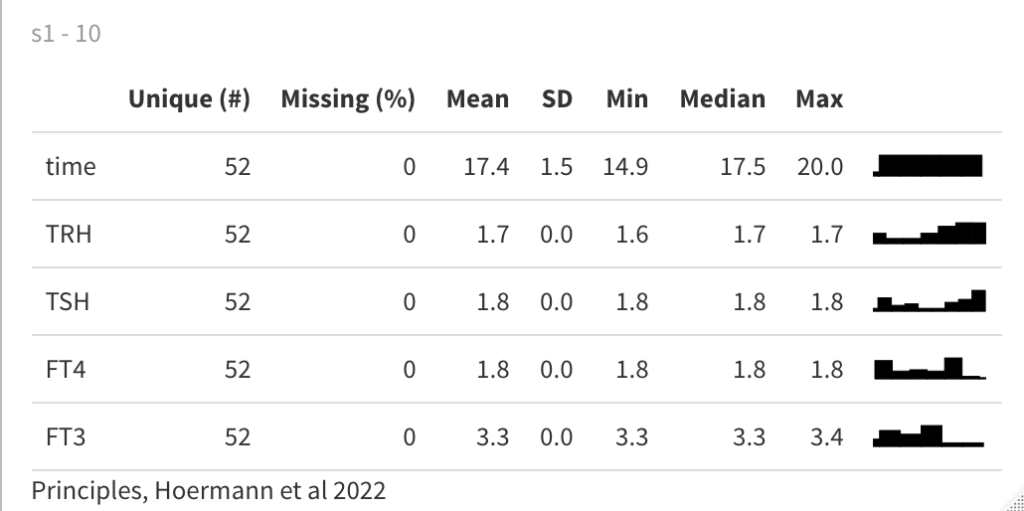
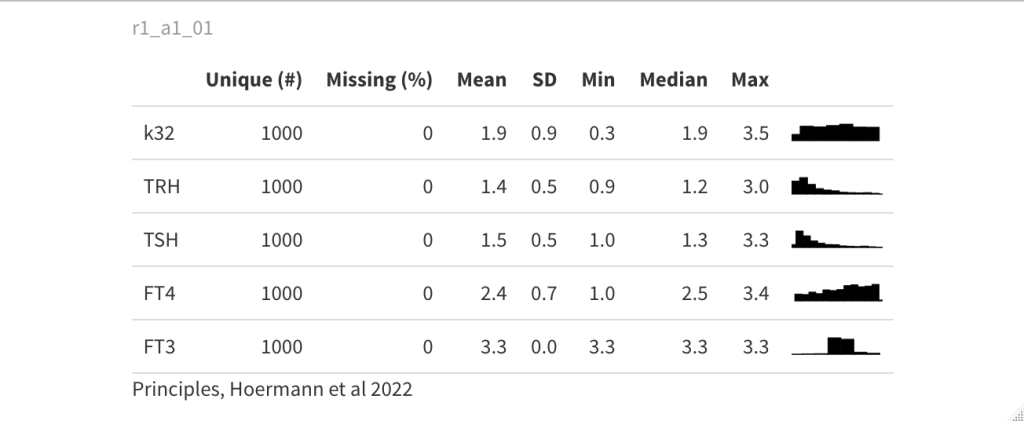
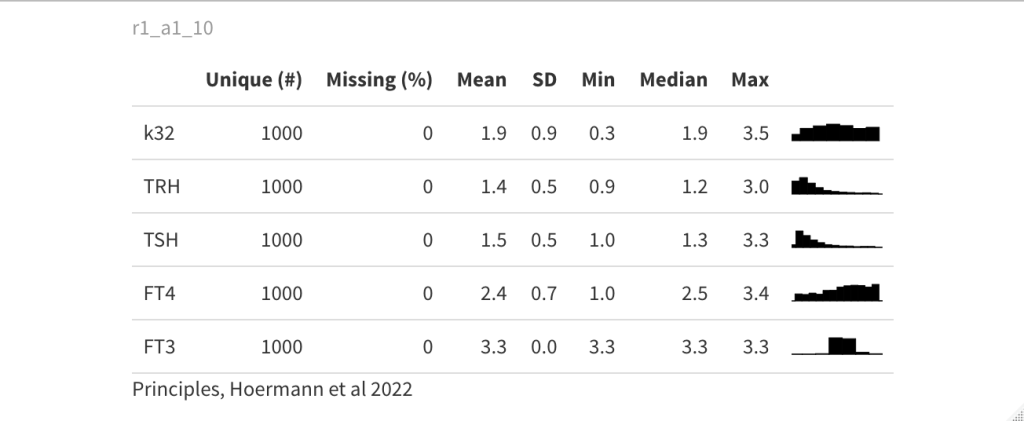
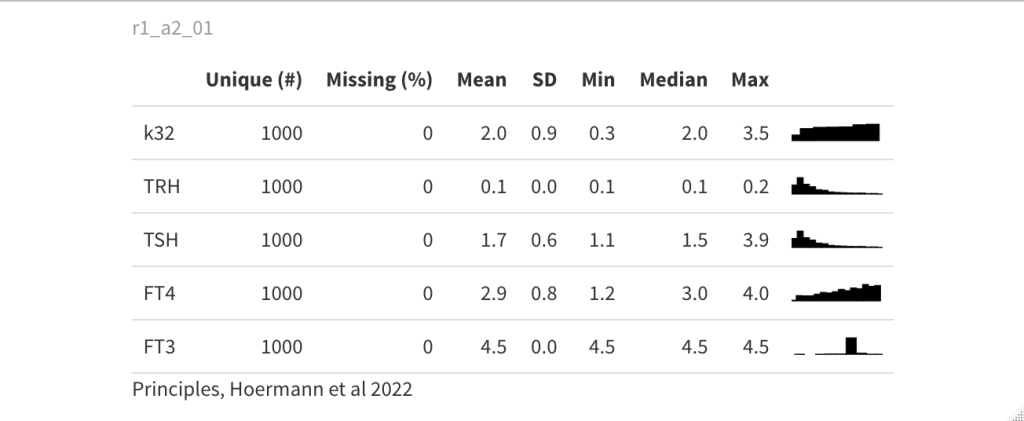
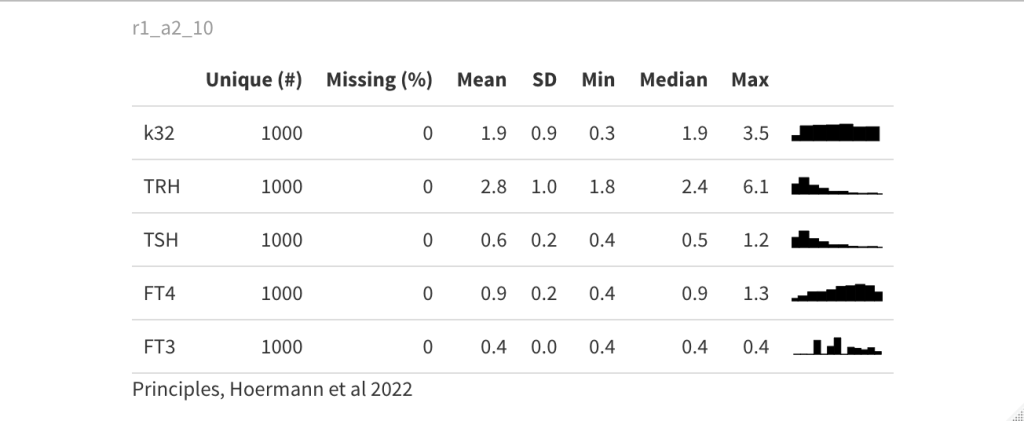
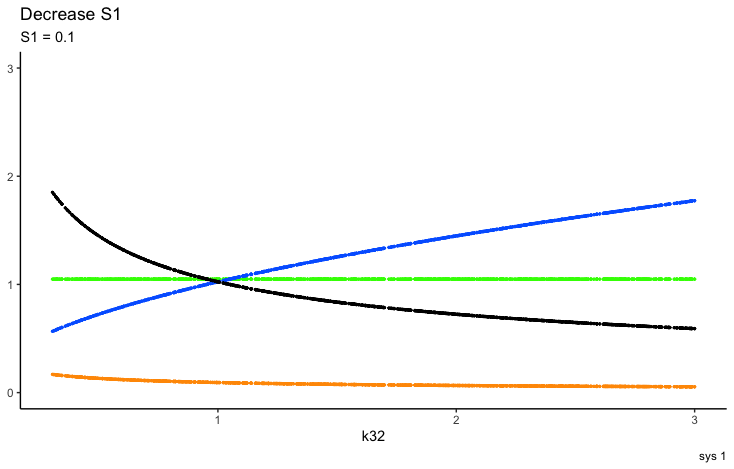
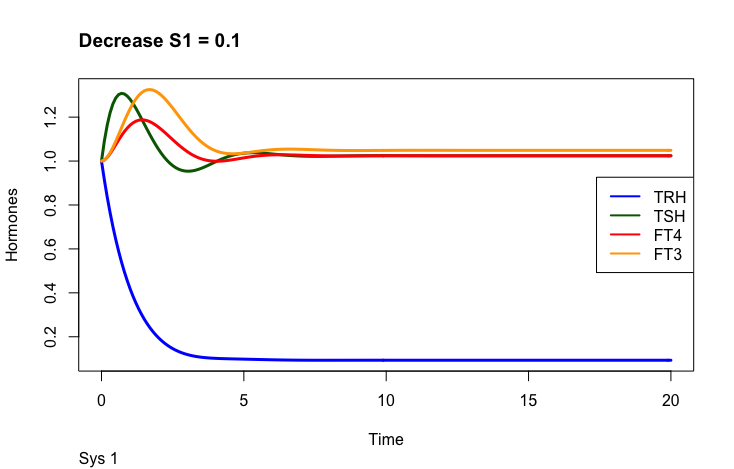
S1 is an input signal with an effect on TRH. As seen in the description above, changes in S1 affect the other hormones as well. The article describes how this knowledge can be used in combination with different parameters.
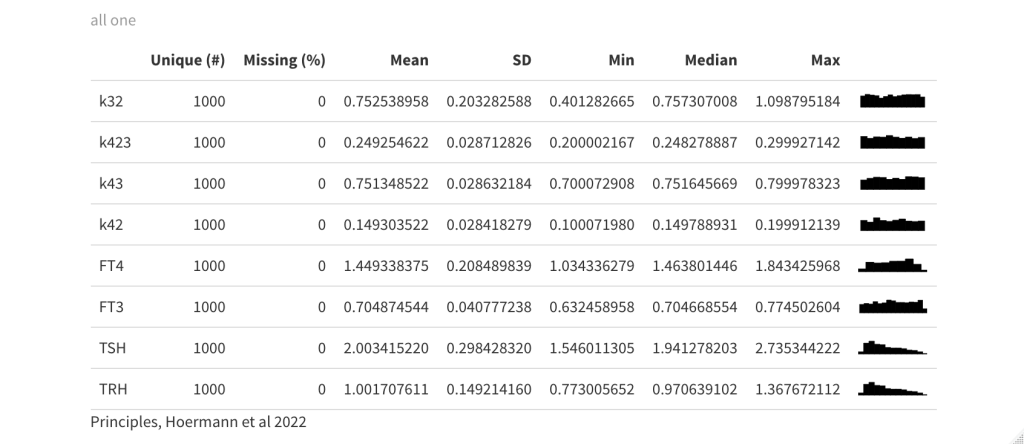
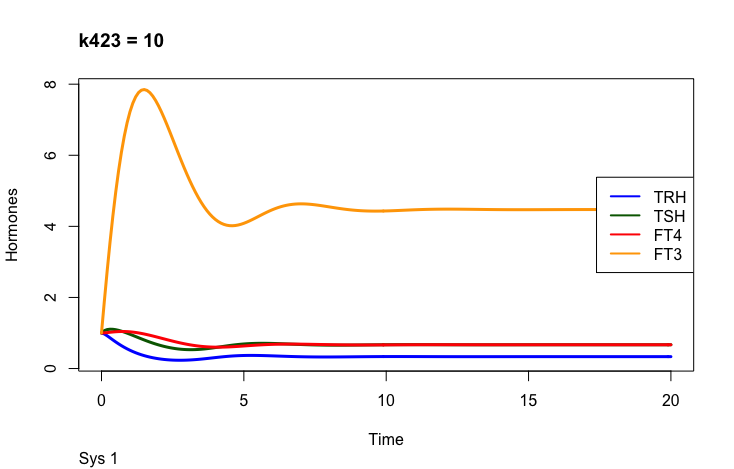
The first part of the above presentation describes the three different equilibrium solutions for s1=1, 0.1 and 10 and the second part describes the time-dependent solution.
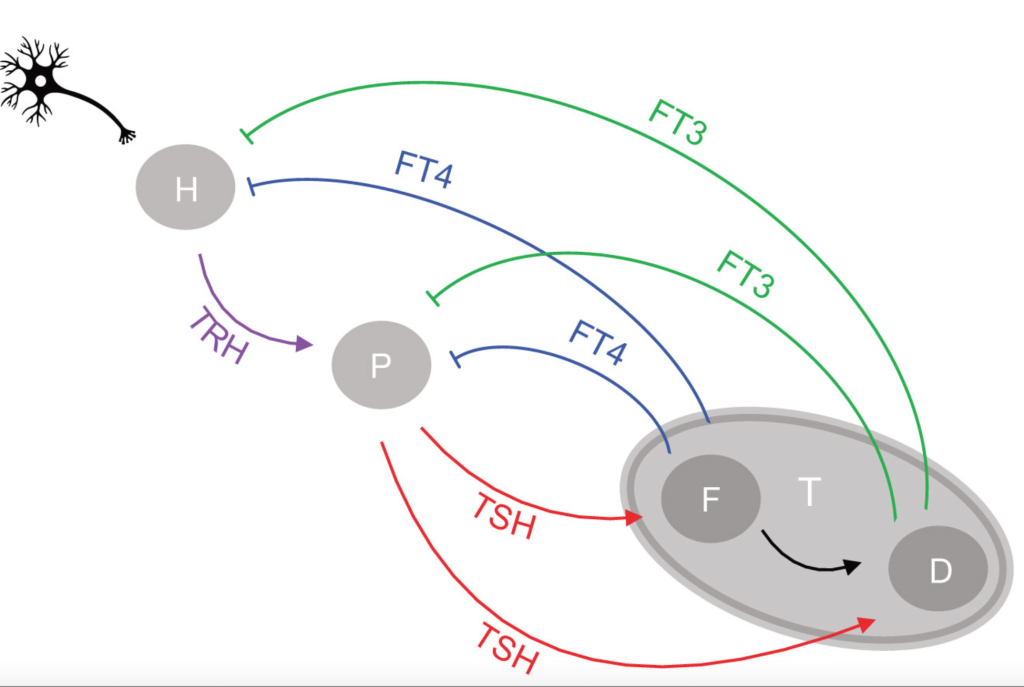
You need not be good at mathematics to see the connection between the used equations and the conceptual drawing of the HPT axis (Ref.1). What is important is the complexity – and flexibility compared to a fixed TSH value as the understanding of the HPT axis.
Overview of the four equationsFig.1 from ref.1 : Network of the hypothalamic-pituitary-thyroid axis regulation
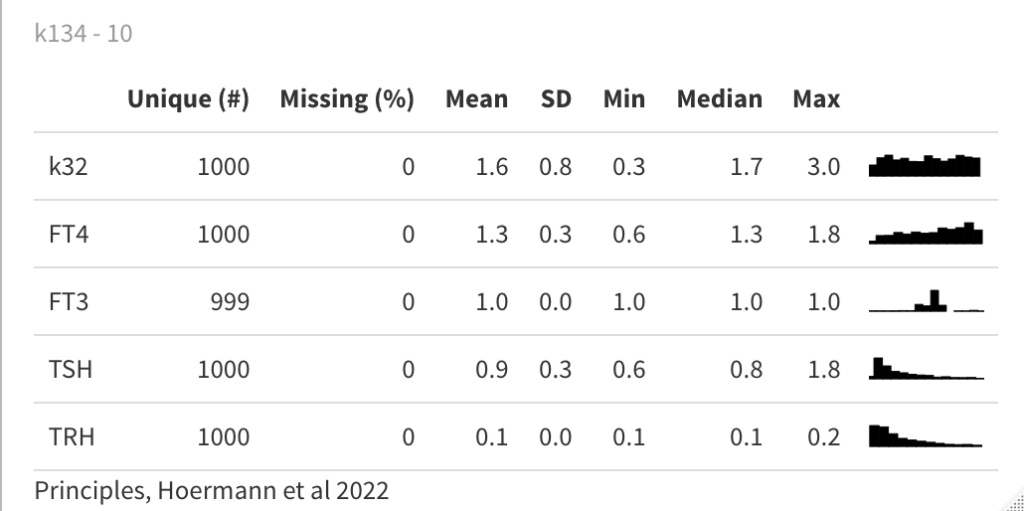
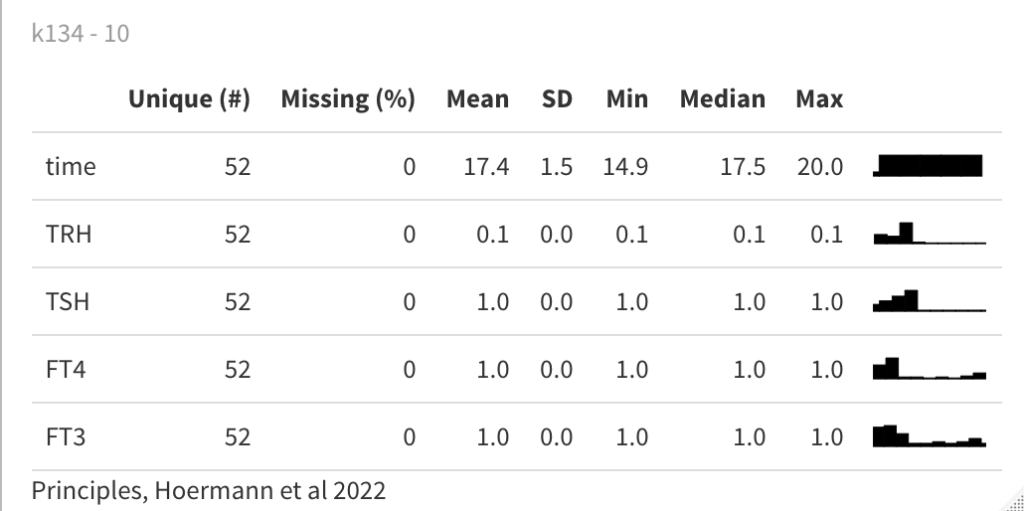
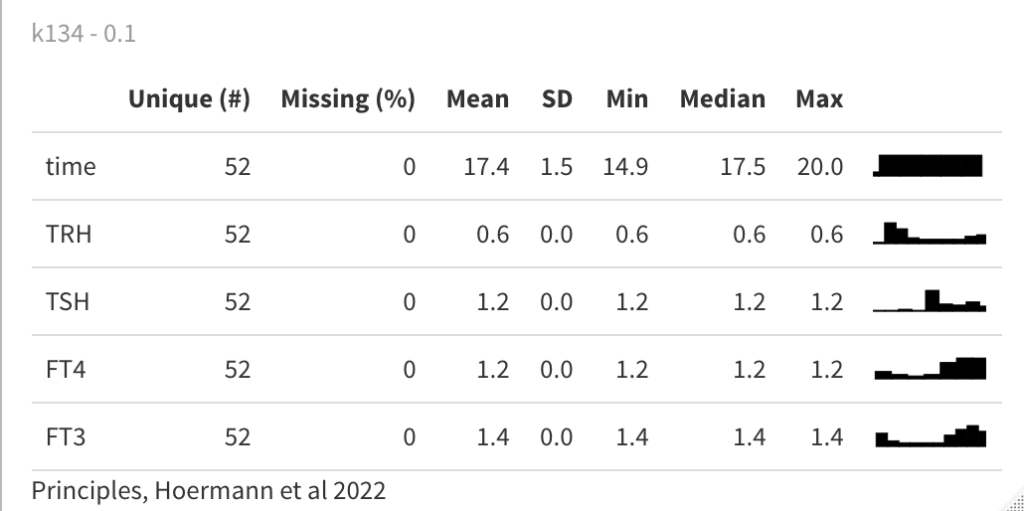
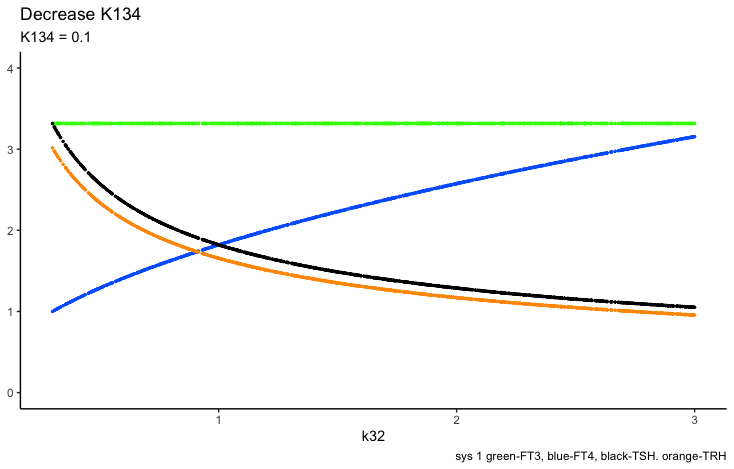
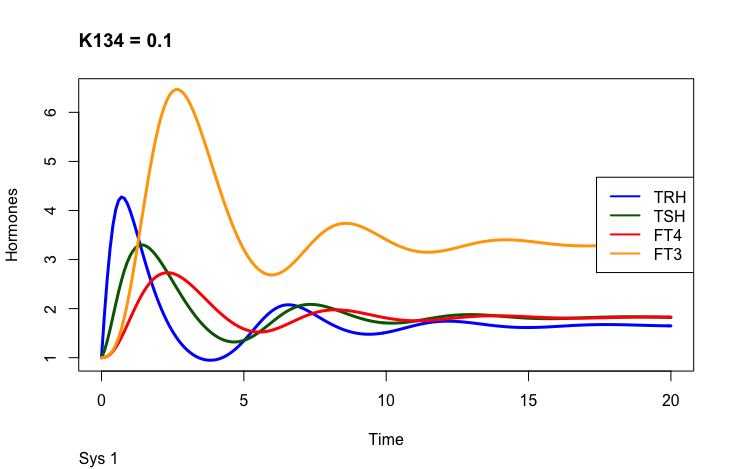
The first part of the second presentation describes the three different equilibrium solutions for k134 =1, 0.1 and 10 and the second part describes the time-dependent solution.
This is theoretical and only serves as an example of how the hormones are changed by the parameter. K134 is the negative feedback of FT4 and FT3 onto TRH (upstream, repressing).
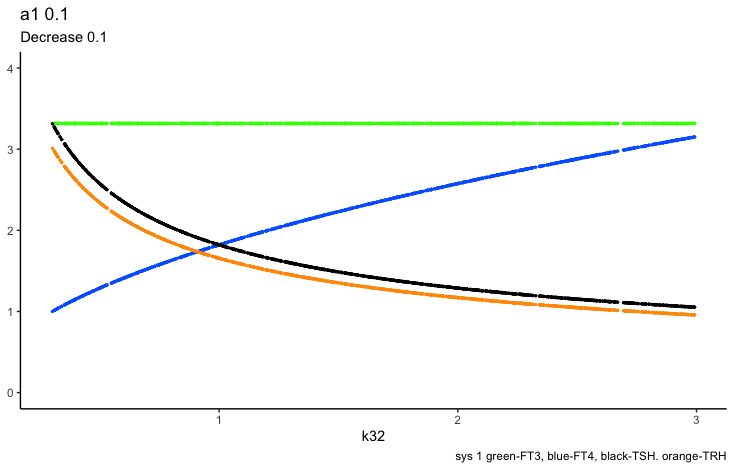
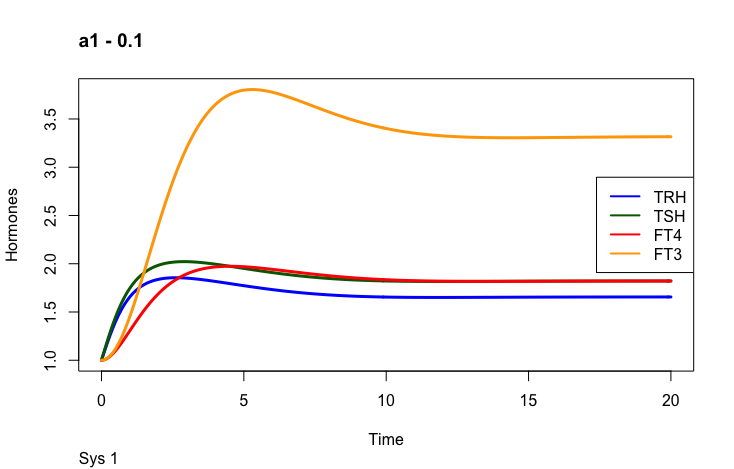
Finally the a1 parameter ( a1 is the TRH elimination rate constant):
a1 parameter
Look at equation 1.1:
We have looked at the effects of s1, k134 and a1 on TRH and the other hormones.
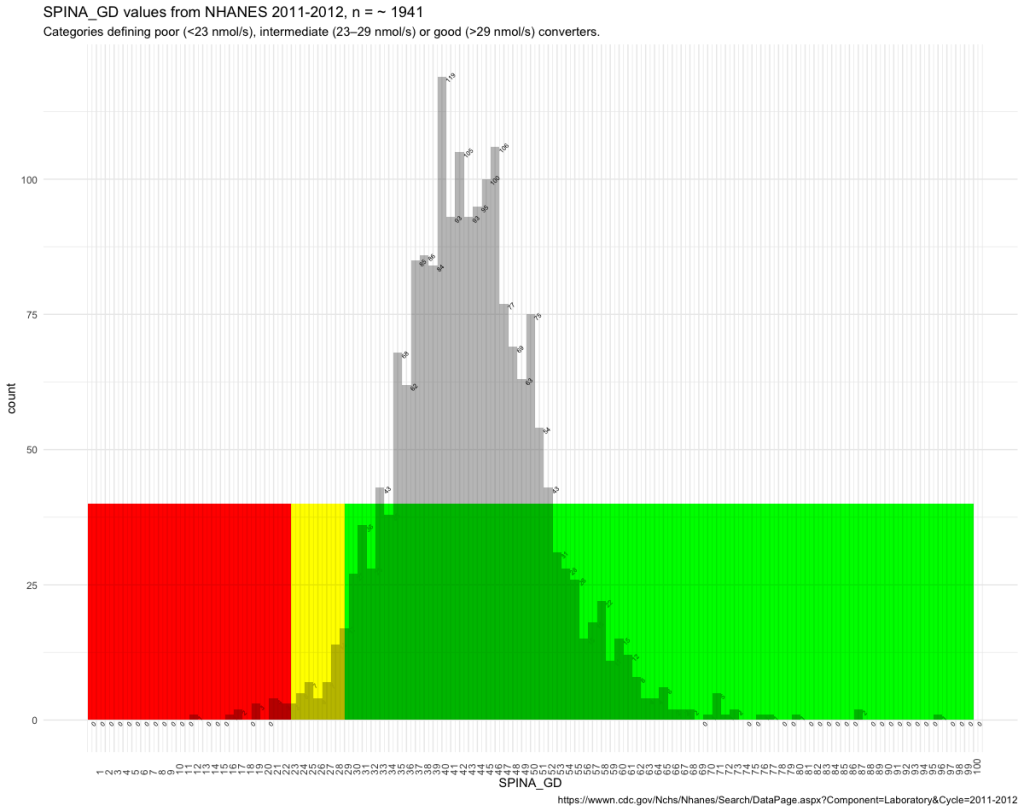
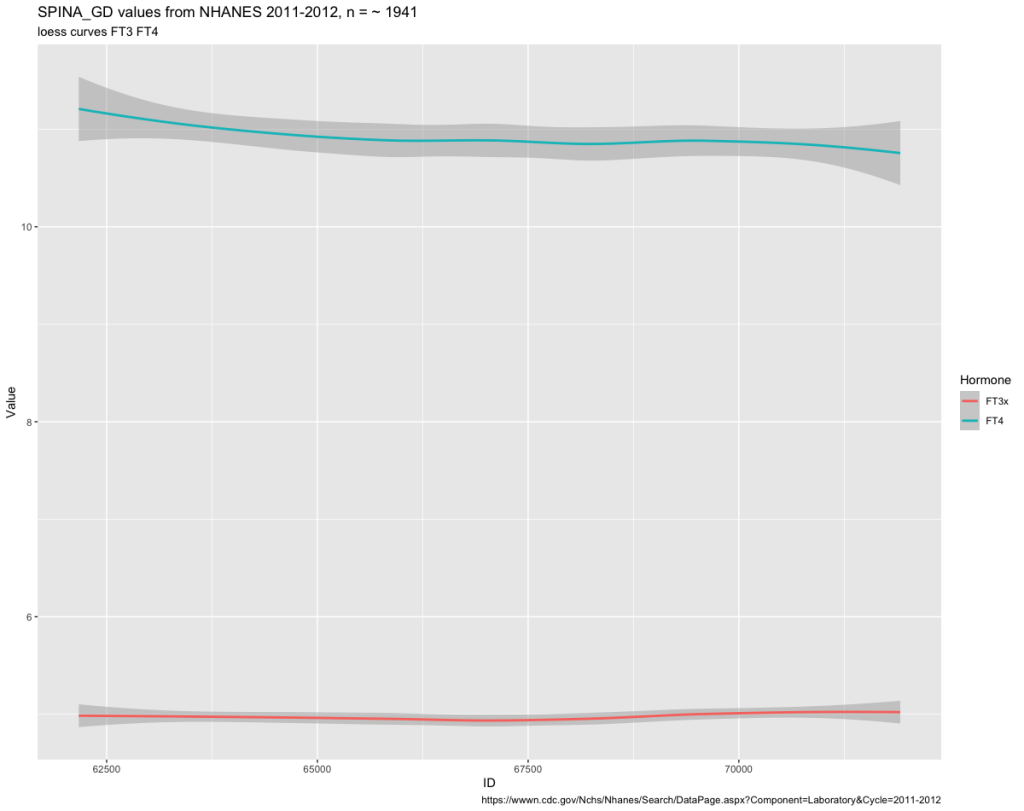
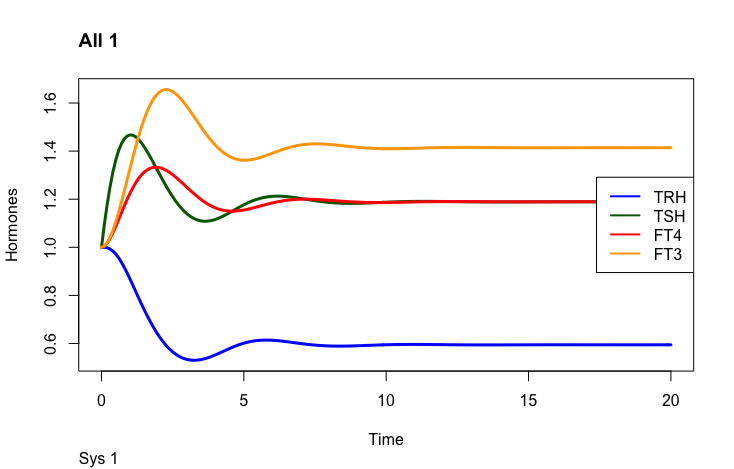
One thing to observe is the FT3 and FT4 curves. In the plot left is shown what the authors call “The perfect homeostasis”. Here the two curves follow each other with a certain distance. In the plots above this pattern is disrupted. We will get back to these observations later.
Hoermann R, Pekker MJ, Midgley JEM, Larisch R and Dietrich JW (2022) Principles of Endocrine Regulation: Reconciling Tensions Between Robustness in Performance and Adaptation to Change. Front. Endocrinol. 13:825107. doi: 10.3389/fendo.2022.825107 https://www.frontiersin.org/articles/10.3389/fendo.2022.825107/full
A study by Zheng 2022, in Frontiers (Ref. 1) looks at how you are able to characterize patients with subclinical hypothyroidism.
Comparison of Five Different Criteria for Diagnosis of Subclinical Hypothyroidism in a Large-Scale Chinese Population:
When an elevated TSH concentration was defined as ≥4.50 mIU/ L,
(1) – an elevated TSH concentration with a normal FT4 concentration,
(2) – an elevated TSH concentration with normal concentrations of FT3 and FT4,
(3) – an elevated TSH concentration with normal concentrations of TT3 and TT4, 35 obs. not shown
(4) – an elevated TSH concentration with normal concentrations of FT4 and TT4
(5) – an elevated TSH concentration with normal concentrations of TT3, TT4, FT3, and FT4.
5
Crit 5
62971
65885
68250
70161
70865
6
Crit 2
62971
65885
66877
68250
70161
70865
7
crit 1
62971
65885
66877
68250
69704
70161
70865
7
Crit 4
62971
65885
66877
68250
69704
70161
70865
Table 1 – ID numbers and criteria
The results shown in table 1 indicate that criteria 5 is the most precise.
ID
AGE
FT3x
FT4
TSH
TT3
TT4x
1
66877
80
4.158
17.7
4.7
1
147.1041
2
69704
30
6.93
13.7
4.66
3
112.3551
Table 2 The T3 values in bold are outside the Chinese reference interval
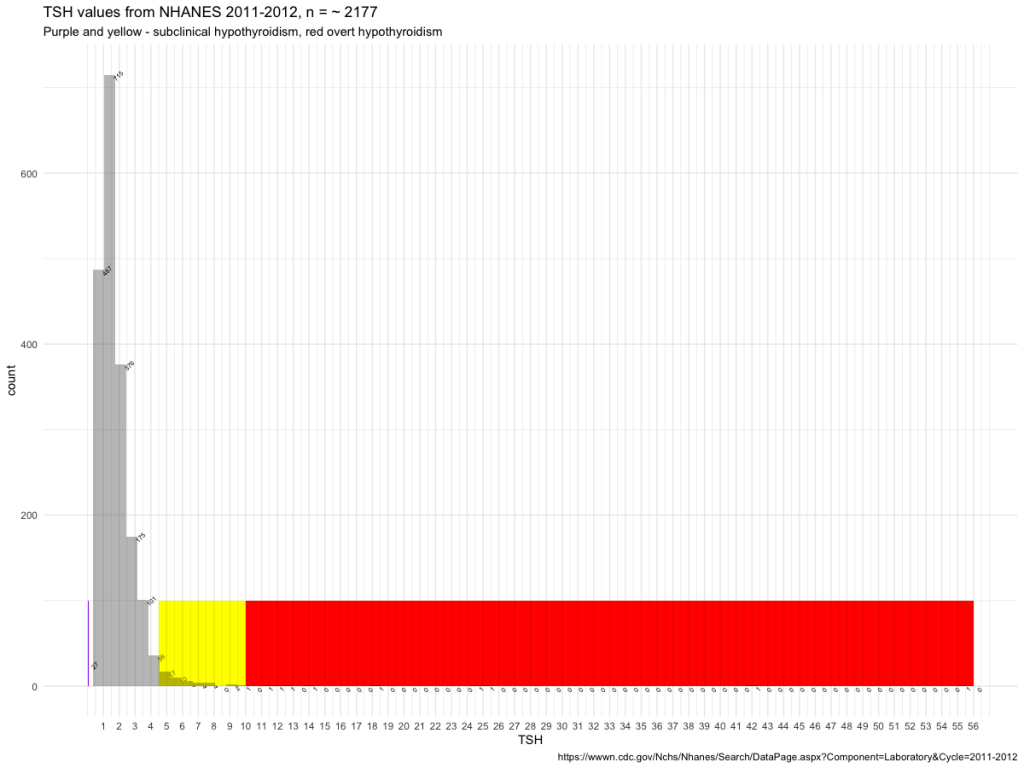
That I have applied these criteria to the NHANES figures (Ref. 2) is of course not reasonable nor science but an attempt to illustrate what they are capable of. To me, it revealed that the reference interval is floating.
Next, I applied the reference intervals from NHANES to the 5 criteria.
The NHANES reference values as a basis – the difference between criteria 1 (28 obs) and criteria 5 (21 obs). The T3 values are important for judging subclinical values better than just for TSH/FT4 values. In table 3 are the 7 persons that differ between criteria 1 and 5.
ID
FT3
FT4
TSH
TT3
TT4
70119
4.01
0.73
7.55
117
6.83
70045
2.67
0.61
12.49
92
5.44
67460
1.73
0.79
11.28
69
8.24
66056
2.21
0.8
5.93
66
7.9
65145
2.29
0.88
42.09
64
7.93
63150
3.31
0.85
6.15
123
5.63
62919
2.98
0.77
7.24
100
5.98
Ref. val
2,5 – 3,9
0.6 – 1.6
80 – 200
6.09 – 12.23
Table 3 – ID numbers and characteristics of combinations of thyroid hormones (Those with TSH > 10 should be excluded – not SCH)
Four of the 7 not excluded would have been found by the FT3 value and only – three of the values would have been found by TT4. This follows the results seen in the Zheng et al article.
5 criteria plus TSH above the upper reference level gives the best result.
There has been a focus on the TSH levels as the indicator of subclinical hypothyroidism if FT4 at the same time in the reference interval. The summary of the FT4 values in criteria 5 is not sufficient in identifying the last seven persons. Only applying the FT3 reference interval identifies the last persons with subclinical hypothyroidism.
There is an ongoing debate on the quality of life of hypothyroid patients. Some 10% of patients report hypothyroid symptoms although they are pharmacologically compensated.
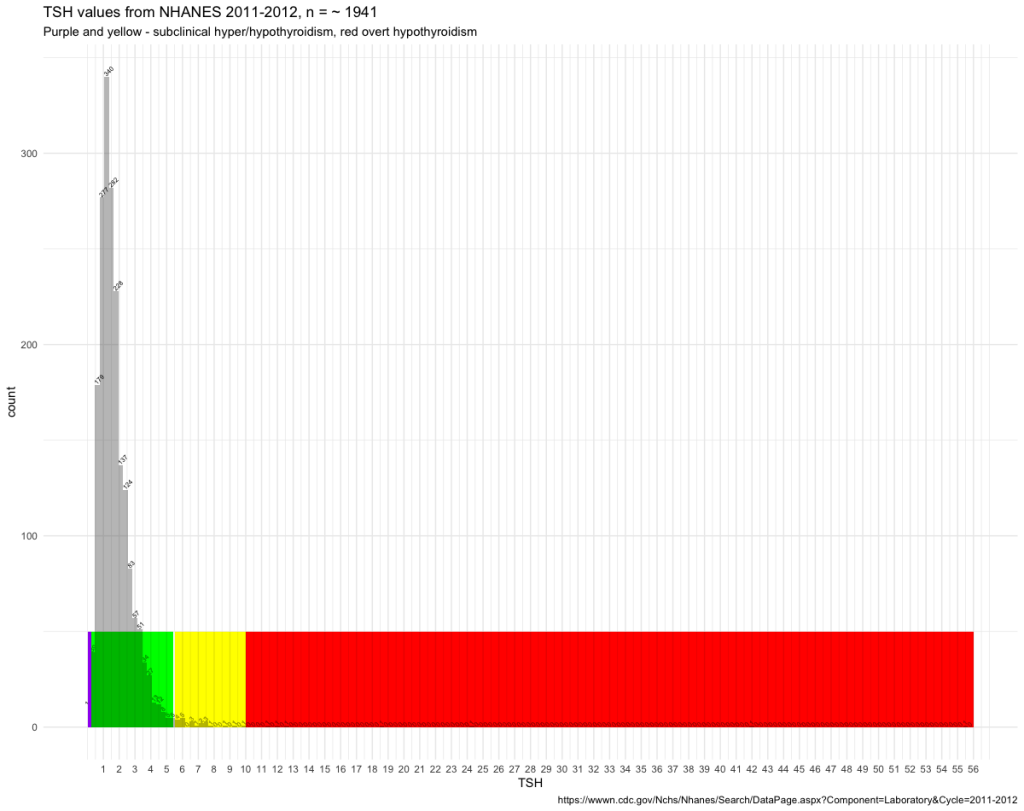
Doctors may have different treatment goals:
When the patients TSH is in the green range they are satisfied with the treatment result.
Others choose a more refined treatment goal:
Seeking the exact thyroid profile that suits the patient.
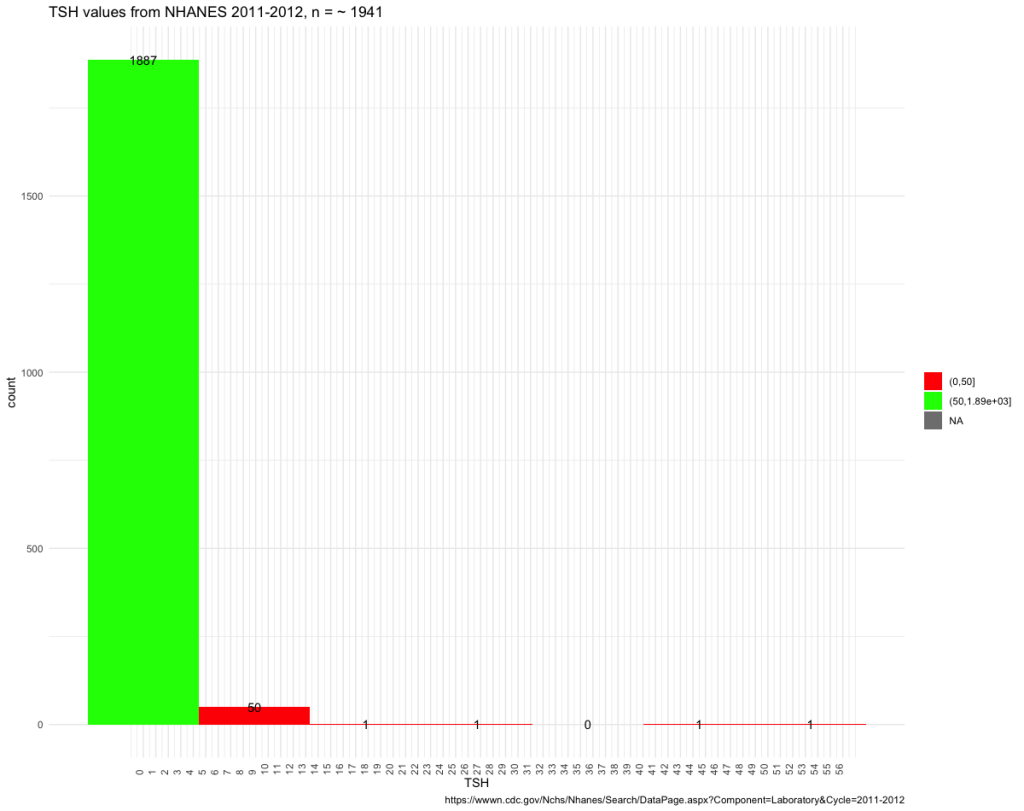
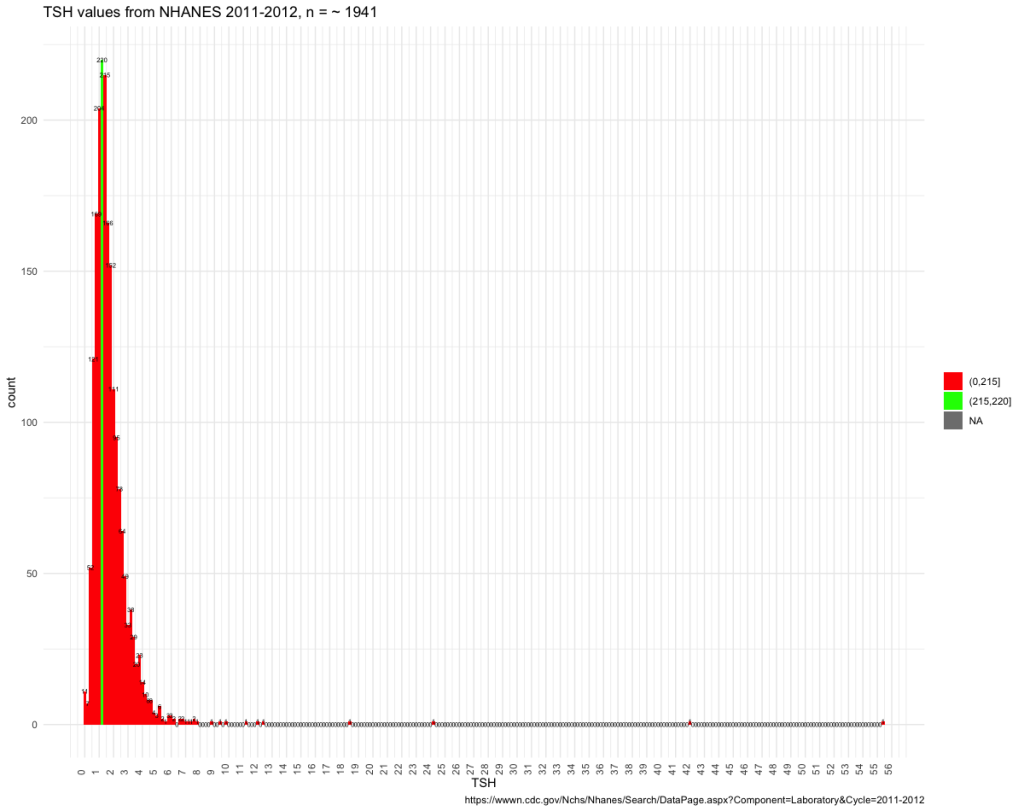
Patients are individual and so are their TSH values.
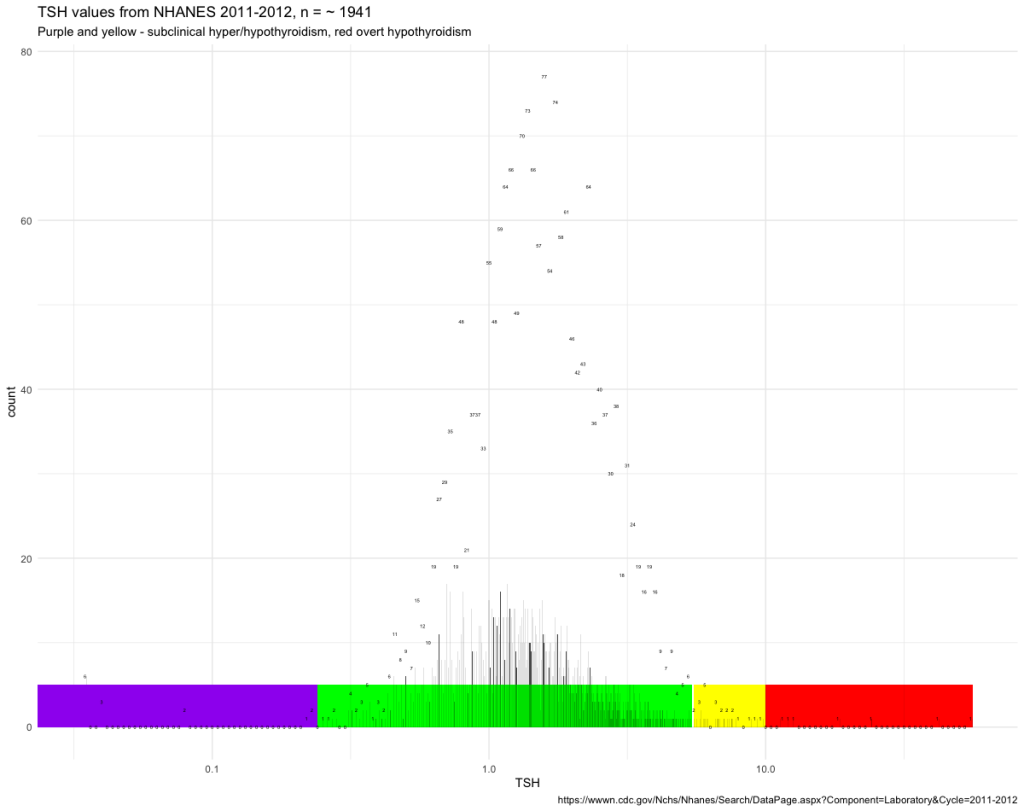
Using another image that has been changed logarithmically shows how few persons you may find in each of the bars:
These images show how individual the TSH values are and that you should not accept an unsuccessful treatment. We have not yet looked at the two important hormones T4 and T3 but I will promise you that they will add to the individuality.
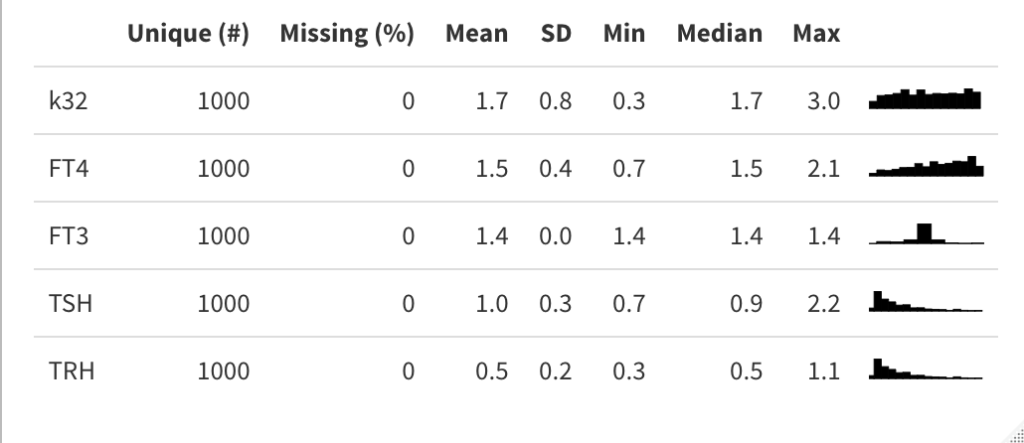
For now two tables with the raw data for the different figures that we will touch upon:
Thyroid Profile in this page – https://wwwn.cdc.gov/Nchs/Nhanes/Search/DataPage.aspx?Component=Laboratory&Cycle=2011-2012
Based on the data the following histogram was created showing counts for different levels of TSH.
Based on the data the following 3D scatterplot was created showing the high individuality of thyroid hormone combinations.
Running a script to identify distinct values showed that TSH, FT3 and FT4 were unique for 1964 observations. For TSH, TT3, TT4 1949 observations were unique.
This shows based on these NHANES data, that the combination of the thyroid hormones is individual. Should treatment be based on averaged values or should the aim be finding the patients previous set-point?


 Hoermann R, Pekker MJ, Midgley JEM, Larisch R and Dietrich JW (2022) Principles of Endocrine Regulation: Reconciling Tensions Between Robustness in Performance and Adaptation to Change. Front. Endocrinol. 13:825107. doi: 10.3389/fendo.2022.825107
Hoermann R, Pekker MJ, Midgley JEM, Larisch R and Dietrich JW (2022) Principles of Endocrine Regulation: Reconciling Tensions Between Robustness in Performance and Adaptation to Change. Front. Endocrinol. 13:825107. doi: 10.3389/fendo.2022.825107